Retroauricular Fissuring: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Retroauricular fissuring refers to painful linear cracks or erosions in the skin behind the ear, commonly associated with inflammatory dermatologic conditions such as seborrheic dermatitis, atopic dermatitis, psoriasis, or contact dermatitis. Although often overlooked, these fissures can cause significant discomfort, secondary infection, and impaired quality of life. Patients typically present with erythema, scaling, itching, and painful fissures in the retroauricular fold. Diagnosis is primarily clinical and supported by dermatological examination and history of associated skin disorders or irritant exposure. Management involves identification of the underlying cause, topical anti-inflammatory therapy, emollients, and prevention of secondary infection. This report describes a case of retroauricular fissuring in an adult patient with chronic seborrheic dermatitis that responded well to topical therapy and supportive care.
Introduction
Retroauricular fissuring is a dermatologic condition characterized by linear cracks in the skin located in the retroauricular fold, the crease behind the external ear. The area is particularly prone to irritation due to moisture retention, friction, and accumulation of sebaceous secretions.
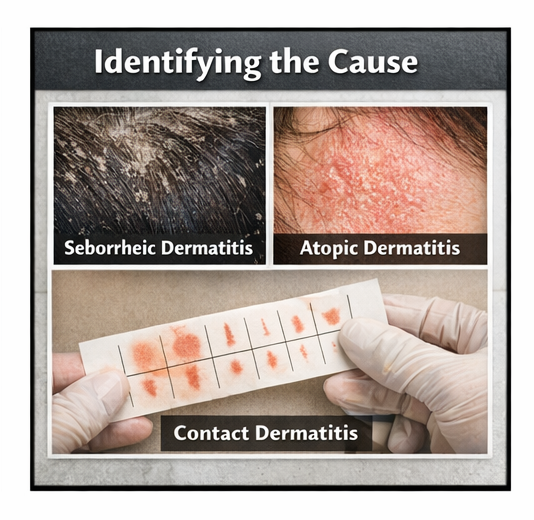
The condition is frequently associated with inflammatory dermatoses, particularly seborrheic dermatitis and atopic dermatitis, but may also occur in psoriasis, allergic contact dermatitis, and fungal infections. Environmental factors such as excessive moisture, poor hygiene, irritation from hair products, or prolonged mask use may contribute to its development.
Pathophysiologically, chronic inflammation and disruption of the skin barrier lead to dryness, scaling, and eventual splitting of the skin surface. The resulting fissures may be painful and predispose patients to secondary bacterial or fungal infections.
Early recognition and treatment are important to relieve symptoms, prevent complications, and address the underlying dermatological disorder. This report presents a case of retroauricular fissuring associated with seborrheic dermatitis that was successfully treated with topical therapy.
Case Report
Patient History
A 35-year-old male presented to the dermatology outpatient clinic with complaints of painful cracks behind both ears for approximately three weeks. The patient reported itching and a mild burning sensation in the affected area, which worsened with sweating and hair washing.

He also noted flaky scaling on the scalp and eyebrows for several months. There was no history of trauma, ear discharge, or recent infection. The patient denied using new cosmetic products or medications.
Past medical history was unremarkable, and there was no known history of psoriasis or atopic dermatitis.
Clinical Examination
On examination, the patient appeared comfortable and afebrile.
Dermatological examination revealed:
• Bilateral erythema in the retroauricular folds
• Linear fissures with mild crusting behind both ears
• Greasy scales extending to the scalp margin
• Mild tenderness on palpation
No cervical lymphadenopathy was noted. Examination of the scalp revealed diffuse scaling suggestive of seborrheic dermatitis.
Clinical Evaluation
Differential Diagnosis
Based on the presenting symptoms and clinical findings, the following conditions were considered:
• Seborrheic dermatitis with retroauricular fissuring
• Atopic dermatitis
• Allergic contact dermatitis
• Psoriasis
• Superficial fungal infection
Further evaluation was undertaken to confirm the diagnosis.
Investigations
Skin Examination
Dermatologic assessment revealed greasy scales over the scalp, eyebrows, and nasolabial folds consistent with seborrheic dermatitis.
Fungal Microscopy
Skin scrapings examined with potassium hydroxide (KOH) preparation did not reveal fungal elements.
These findings supported the diagnosis of retroauricular fissuring secondary to seborrheic dermatitis.
Diagnosis
Based on clinical findings and exclusion of fungal infection, a diagnosis of retroauricular fissuring associated with seborrheic dermatitis was established.
Management and Outcome
Initial Management
The patient was treated with conservative and topical therapy including:
• Topical low-potency corticosteroid cream applied to the fissured area

• Ketoconazole-containing antifungal shampoo for scalp involvement
• Emollient cream applied twice daily to restore skin barrier function

• Advice to avoid harsh shampoos and irritant hair products
Follow-Up and Outcome
At two-week follow-up, the patient reported significant reduction in itching and pain.
Clinical improvements included:
• Healing of retroauricular fissures
• Reduction in erythema and scaling
• No evidence of secondary infection
After four weeks of therapy, the fissures had completely healed and scalp scaling had markedly improved. The patient was advised to continue maintenance therapy with medicated shampoo and regular moisturization.

Discussion
Retroauricular fissuring is a relatively common but often underrecognized dermatologic manifestation associated with inflammatory skin diseases. The retroauricular fold is particularly susceptible to irritation because of its moist environment and frequent exposure to friction.
Seborrheic dermatitis is one of the most frequent underlying causes. It is a chronic inflammatory disorder associated with sebaceous gland activity and colonization by Malassezia species. Inflammation and scaling may extend beyond the scalp to involve the eyebrows, nasolabial folds, and retroauricular region.
Clinically, retroauricular fissures present as painful linear cracks in erythematous skin, often accompanied by scaling or crusting. Persistent fissures may predispose patients to secondary bacterial infection.
Diagnosis is primarily clinical, supported by dermatologic examination and exclusion of fungal infections or allergic reactions. Management focuses on treating the underlying inflammatory condition while restoring the skin barrier.
Topical corticosteroids, antifungal therapy, and emollients are commonly used treatments. Appropriate skin care practices and avoidance of irritants also play an important role in preventing recurrence.
Conclusion
Retroauricular fissuring is a dermatologic condition characterized by painful linear cracks in the skin behind the ear and is commonly associated with inflammatory skin disorders such as seborrheic dermatitis. Although often considered minor, it can cause significant discomfort and may predispose patients to secondary infection if untreated.
Accurate diagnosis based on clinical examination and appropriate investigations is essential for effective management. Treatment typically involves topical anti-inflammatory therapy, antifungal agents when indicated, and consistent use of emollients to restore skin barrier function.
Early recognition and appropriate treatment can lead to rapid symptom relief, complete healing of retroauricular fissures, and effective prevention of recurrence. Prompt identification of the underlying dermatologic condition such as seborrheic dermatitis, atopic dermatitis, or contact dermatitis allows clinicians to initiate targeted therapy, including topical anti-inflammatory agents, antifungal treatments when indicated, and regular use of emollients to restore the skin barrier. In addition, patient education regarding proper skin care, avoidance of irritants, and maintenance therapy plays a crucial role in preventing repeated episodes. With timely diagnosis, appropriate medical management, and consistent follow-up, most patients experience significant clinical improvement, restoration of normal skin integrity, and a reduced risk of complications such as secondary infection or chronic skin irritation.
References
- Clark GW, Pope SM, Jaboori KA. Diagnosis and treatment of seborrheic dermatitis. American Family Physician. 2015. https://pubmed.ncbi.nlm.nih.gov/25822272/
- Dessinioti C, Katsambas A. Seborrheic dermatitis: etiology, risk factors, and treatments. Clinics in Dermatology. 2013. https://pubmed.ncbi.nlm.nih.gov/23159109/
- Borda LJ, Wikramanayake TC. Seborrheic dermatitis and dandruff: a comprehensive review. Journal of Clinical and Investigative Dermatology. 2015. https://pubmed.ncbi.nlm.nih.gov/27148560/
- Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. The Lancet. 2020. https://pubmed.ncbi.nlm.nih.gov/32422179/
- Naldi L, Rebora A. Seborrheic dermatitis. New England Journal of Medicine. 2009. https://pubmed.ncbi.nlm.nih.gov/19587340/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
CD39 Blockade Shows Potential in Early-Stage Lung Cancer
2.
Q&A: Researchers discuss identifying potential new protein targets for melanoma therapeutics
3.
PFS in Multiple Myeloma Is Improved by Daratumumab Added to Standard Therapy.
4.
Venetoclax Combo Shows Promise in Younger Patients With AML
5.
Long Wait Times on the Other Side of the Pond: King Charles' Cancer Diagnosis.
1.
Understanding SVR Normal Range: A Guide to Achieving Optimal Health
2.
Engineering the Future of Oncology with CAR- Natural Killer Cell Design & Therapeutics
3.
Hope in Numbers: Understanding AML Leukemia Survival Rates and Emerging Therapies
4.
Boosting Checkpoint Immunotherapy in Hodgkin Lymphoma with JAK Inhibition: Advances & Insights
5.
CAR-T Cell Therapy for B-Cell Acute Lymphoblastic Leukemia: A Comprehensive Review
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Newer Immunotherapies for Myeloma- A Comprehensive Overview
2.
An Eagles View - Evidence-based Discussion on Iron Deficiency Anemia- Panel Discussion III
3.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part V
4.
Molecular Contrast: EGFR Axon 19 vs. Exon 21 Mutations - Part II
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part III

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge