Pyogenic Liver Abscess: Clinical Presentation, Diagnostic Evaluation, Management, and Outcome – A Case Report
OthersPage Navigation
Abstract
Pyogenic liver abscess (PLA) is a potentially life-threatening intra-abdominal infection characterized by the accumulation of pus within the liver parenchyma. Although advances in imaging, antimicrobial therapy, and interventional radiology have significantly improved outcomes, delayed diagnosis may lead to severe complications including sepsis, rupture, and multi-organ failure. Common causative organisms include Escherichia coli, Klebsiella pneumoniae, Streptococcus species, and anaerobic bacteria. Clinical presentation is often nonspecific, making early recognition challenging.
We present the case of a 52-year-old male who presented with fever, right upper quadrant abdominal pain, and generalized weakness. Laboratory investigations revealed leukocytosis and elevated inflammatory markers. Ultrasonography and contrast-enhanced computed tomography demonstrated a large pyogenic abscess in the right hepatic lobe. Blood cultures identified Klebsiella pneumoniae. The patient was successfully managed with intravenous antibiotics and ultrasound-guided percutaneous drainage, resulting in complete clinical recovery.
This case highlights the importance of prompt diagnosis, appropriate microbiological evaluation, imaging-guided intervention, and multidisciplinary management in achieving favorable outcomes in pyogenic liver abscess.
Introduction
Pyogenic liver abscess is the most common visceral abscess and represents a serious infectious condition requiring timely diagnosis and treatment. It occurs when bacteria invade the liver through the biliary tract, portal circulation, hepatic artery, direct extension from adjacent structures, or traumatic injury.
Predisposing factors include:
• Diabetes mellitus
• Biliary tract disease
• Cholangitis
• Intra-abdominal infections
• Immunosuppression
• Malignancy
• Liver trauma
Common pathogens include:
• Klebsiella pneumoniae
• Escherichia coli
• Streptococcus species
• Enterococcus species
• Anaerobic bacteria
Clinical manifestations often include fever, abdominal pain, malaise, anorexia, and weight loss. Because symptoms are frequently nonspecific, imaging studies play a critical role in establishing the diagnosis.
Early intervention is essential to prevent severe complications and mortality.
Case Report
Patient History
A 52-year-old male presented to the emergency department with complaints of:
• High-grade fever for 10 days
• Right upper abdominal pain for 1 week
• Loss of appetite
• Generalized weakness
• Intermittent chills and rigors
The abdominal pain was dull, continuous, and localized to the right hypochondrium.
The patient denied:
• Vomiting
• Jaundice
• Gastrointestinal bleeding
• Recent travel
• Tuberculosis exposure
Past medical history revealed:
• Type 2 diabetes mellitus for 8 years
• Hypertension for 5 years
There was no history of liver disease or alcohol abuse.
Clinical Examination
General Examination
• Blood pressure: 132/84 mmHg
• Pulse rate: 104/min
• Respiratory rate: 20/min
• Temperature: 101.8°F
• Oxygen saturation: 98% on room air
The patient appeared ill and mildly dehydrated.
Systemic Examination
Abdominal examination revealed:
• Right upper quadrant tenderness
• Mild hepatomegaly
• No guarding
• No rigidity
• No ascites
Cardiovascular and respiratory examinations were unremarkable.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Pyogenic liver abscess
• Amoebic liver abscess
• Acute cholecystitis
• Hepatic malignancy
• Liver cyst infection
• Subphrenic abscess
The presence of fever, leukocytosis, and localized hepatic tenderness strongly suggested an infective hepatic process.
Investigations
Laboratory Evaluation
Routine investigations revealed:
• Hemoglobin: 11.8 g/dL
• Total leukocyte count: 17,600/mm³
• Platelet count: 328,000/mm³
• ESR: 58 mm/hr
• CRP: 142 mg/L
Liver function tests showed:
• Total bilirubin: 1.2 mg/dL
• AST: 72 U/L
• ALT: 68 U/L
• Alkaline phosphatase: 245 U/L
Blood glucose levels were elevated.
Blood Cultures
Blood cultures demonstrated:
• Klebsiella pneumoniae growth
• Sensitivity to ceftriaxone and piperacillin-tazobactam
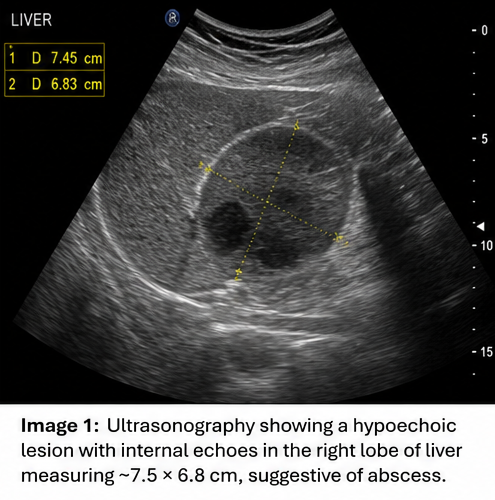
Ultrasonography
Abdominal ultrasonography revealed:
• Hypoechoic lesion in the right hepatic lobe
• Size: 7.5 × 6.8 cm
• Internal echoes suggestive of pus collection
• Mild surrounding edema
Findings were highly suggestive of a liver abscess.
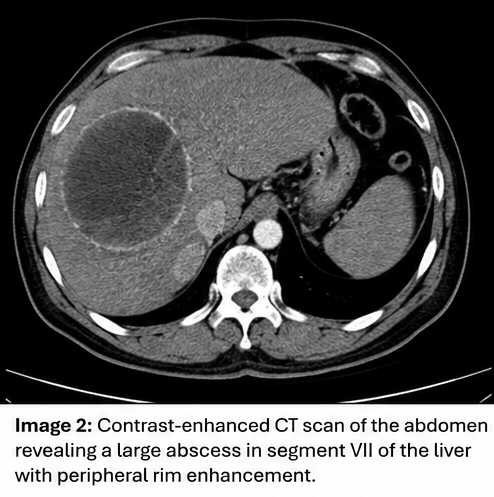
Contrast-Enhanced CT Scan
CT abdomen demonstrated:
• Solitary abscess cavity in segment VII
• Peripheral rim enhancement
• Central low-density necrotic content
• No rupture
• No intra-abdominal collections
Diagnosis
Based on clinical findings, laboratory investigations, imaging studies, and blood culture results, a diagnosis of: Pyogenic Liver Abscess Caused by Klebsiella pneumonia was established.
Management and Outcome
Initial Management
The patient was admitted and started on:
• Intravenous fluids
• Glycemic control
• Broad-spectrum intravenous antibiotics
• Supportive care
Empirical therapy included:
• Piperacillin-tazobactam
• Metronidazole
Antibiotics were later adjusted according to culture sensitivity.
Percutaneous Drainage
Because the abscess exceeded 5 cm in diameter, ultrasound-guided percutaneous catheter drainage was performed.
Approximately:
• 180 mL thick purulent material was aspirated.

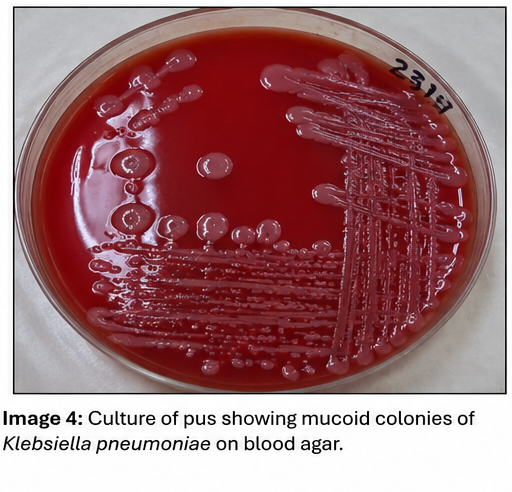
Pus culture confirmed:
• Klebsiella pneumoniae
Hospital Course
At 72 Hours
• Fever subsided
• Pain improved
• Leukocyte count decreased
At 1 Week
• Significant clinical improvement
• Improved appetite
• Reduced inflammatory markers
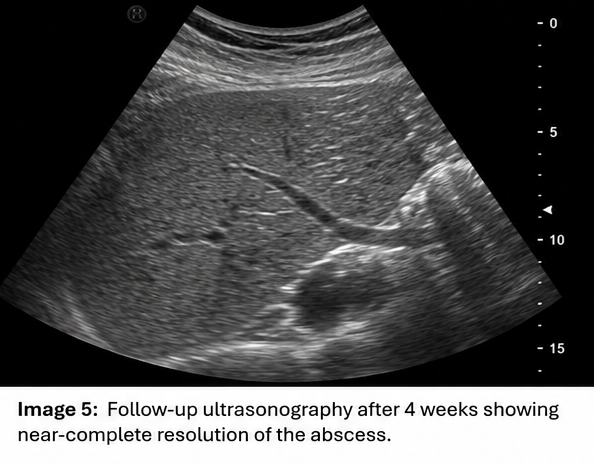
At 2 Weeks
• Drain output minimal
• Follow-up imaging showed cavity reduction
Drain removal was performed successfully.
Follow-Up
At 1 Month
• Complete symptom resolution
• Normal inflammatory markers
• Improved glycemic control
At 3 Months
• No residual abscess
• Normal liver architecture
• Return to normal daily activities
Discussion
Pathophysiology
Pyogenic liver abscess develops when microorganisms invade hepatic tissue and trigger an inflammatory response leading to tissue necrosis and pus formation.
Routes of infection include:
• Biliary spread
• Portal venous spread
• Hematogenous dissemination
• Direct extension
• Traumatic inoculation
Diabetes mellitus significantly increases susceptibility to infection.
Epidemiology
Important epidemiological features include:
• More common in middle-aged adults
• Higher incidence in diabetic patients
• Increased prevalence in Asian populations
• Rising incidence of Klebsiella-associated abscesses
• Male predominance
Clinical Manifestations
Common symptoms include:
• Fever
• Chills
• Right upper quadrant pain
• Weight loss
• Anorexia
• Malaise
Advanced disease may result in:
• Sepsis
• Septic shock
• Abscess rupture
• Pleural complications
Diagnostic Considerations
Diagnosis relies on:
- Clinical suspicion
- Laboratory markers
- Blood cultures
- Ultrasonography
- CT imaging
- Microbiological evaluation
CT imaging remains the gold standard for defining abscess size, location, and complications.
Treatment Modalities
Medical Therapy
Small abscesses may respond to:
• Intravenous antibiotics
• Culture-guided therapy
Image-Guided Drainage
Recommended for:
• Abscesses >5 cm
• Persistent symptoms
• Failure of medical therapy
Surgical Intervention
Reserved for:
• Ruptured abscess
• Multiple complex collections
• Failure of percutaneous drainage
Complications
Potential complications include:
• Septicemia
• Rupture into the peritoneal cavity
• Pleural empyema
• Hepatic failure
• Multi-organ dysfunction
Prompt diagnosis significantly reduces morbidity and mortality.
Prognosis
Prognosis depends upon:
• Early diagnosis
• Organism virulence
• Abscess size
• Comorbid conditions
• Timeliness of drainage
Most patients experience excellent outcomes with modern antibiotic therapy and image-guided drainage.
Conclusion
Pyogenic liver abscess remains a potentially serious but treatable infectious disease. Careful clinical evaluation, timely imaging, microbiological identification, and appropriate drainage procedures are essential for successful management. This case demonstrates the effective treatment of a Klebsiella pneumoniae pyogenic liver abscess through early diagnosis, targeted antimicrobial therapy, and ultrasound-guided percutaneous drainage. Prompt recognition and multidisciplinary management remain crucial for preventing complications and ensuring favorable long-term outcomes.
For a professional case report, you can include the following references in Vancouver style:
References
- Longworth S, Han J. Pyogenic liver abscess. Clinical Liver Disease. 2015;6(2):51-54. https://aasldpubs.onlinelibrary.wiley.com/doi/full/10.1002/cld.476
- Serraino C, Elia C, Bracco C, et al. Characteristics and management of pyogenic liver abscess: A European experience. Medicine (Baltimore). 2018;97(19):e0628. https://journals.lww.com/md-journal/fulltext/2018/05110/characteristics_and_management_of_pyogenic_liver.53.aspx
- Johannsen EC, Sifri CD, Madoff LC. Pyogenic liver abscesses. Infectious Disease Clinics of North America. 2000;14(3):547-563. https://www.sciencedirect.com/science/article/pii/S0891552005701203
- Akhondi H, Sabih DE. Pyogenic Liver Abscess. StatPearls Publishing. Updated 2025. https://www.ncbi.nlm.nih.gov/books/NBK538230/
- Lardière-Deguelte S, Ragot E, Amroun K, et al. Hepatic abscess: Diagnosis and management. Journal of Visceral Surgery. 2015;152(4):231-243. https://www.sciencedirect.com/science/article/pii/S1878788615000283
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Inner Thoughts of Leonard Bernstein, the "Maestro".
2.
Mobile prostate cancer screening clinic can ID the disease in disadvantaged men
3.
No Survival Benefit Seen With Adjuvant Atezolizumab in TNBC
4.
Parents, teachers at Missouri school want answers after string of cancer diagnoses
5.
A promising medication could slow brain tumors in children.
1.
Future-Ready Cancer Screening: What Every Clinician Should Know in 2025
2.
Cancer Evolution and Therapeutic Resistance: Mechanisms, Clinical Insights, and Emerging Strategies
3.
Targeting Cancer Stem Cells in Solid Tumors: Mechanisms, Clinical Implications, and Therapeutic Advances
4.
Partial Gland Ablation in Prostate Cancer: Oncologic Outcomes in Intermediate-Risk Cases
5.
Generative AI for Adaptive Oncology Trial Design
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Management of 1st line ALK+ mNSCLC (CROWN TRIAL Update) - Part III
2.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part I
3.
Recent Data Analysis for First-Line Treatment of ALK+ NSCLC
4.
INO-VATE: The Long-Term Overall Survival Analysis in Iontuzumab-Treated Patients
5.
Current Scenario of Cancer- The Incidence of Cancer in Men

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge