Stenosis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Stenosis refers to the abnormal narrowing of a body passage or tubular structure, leading to impaired blood flow, airflow, or fluid movement. Depending on the affected organ system, stenosis can result in severe functional compromise and life-threatening complications. Among the various forms, lumbar spinal stenosis is a common degenerative condition affecting the elderly population and is characterized by narrowing of the spinal canal resulting in compression of neural structures.
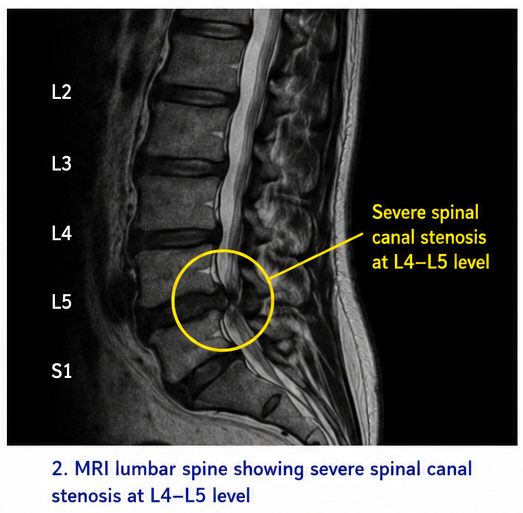
We present the case of a 62-year-old male who presented with chronic lower back pain, progressive bilateral lower limb numbness, and neurogenic claudication affecting mobility for nearly two years. Magnetic resonance imaging (MRI) revealed severe lumbar spinal canal stenosis at the L4–L5 level associated with ligamentum flavum hypertrophy and degenerative disc disease. The patient was managed with conservative therapy initially, followed by decompressive laminectomy due to worsening symptoms and impaired quality of life. Significant symptomatic and functional improvement was observed postoperatively.
This case highlights the importance of early diagnosis, appropriate imaging evaluation, individualized treatment planning, and timely surgical intervention in achieving favorable outcomes in patients with spinal stenosis.
Introduction
Spinal stenosis is a degenerative musculoskeletal disorder characterized by narrowing of the spinal canal, lateral recesses, or neural foramina, resulting in compression of the spinal cord or nerve roots. The condition most commonly affects the cervical and lumbar regions of the spine, with lumbar spinal stenosis being the most prevalent form among older adults.
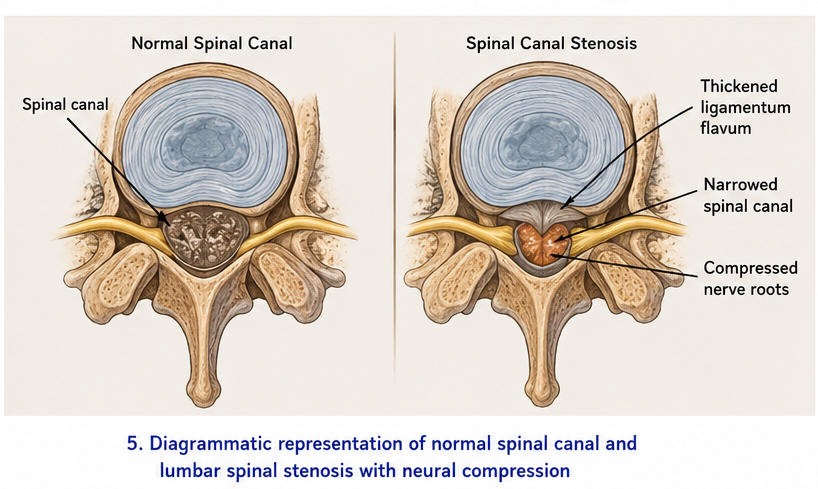
The disease commonly develops due to age-related degenerative changes including intervertebral disc degeneration, osteophyte formation, facet joint hypertrophy, and thickening of the ligamentum flavum. Progressive narrowing of the spinal canal can lead to neurological symptoms, pain, and mobility impairment.
Lumbar spinal stenosis represents one of the leading causes of disability and spinal surgery among the elderly population worldwide.
Important risk factors include:
• Increasing age
• Degenerative disc disease
• Obesity
• Osteoarthritis
• Congenital narrow spinal canal
• Previous spinal injury
• Repetitive spinal stress
• Poor posture and sedentary lifestyle
• Smoking
• Osteoporosis
Common symptoms include:
• Chronic lower back pain
• Neurogenic claudication
• Bilateral lower limb numbness
• Tingling sensations
• Weakness in lower extremities
• Difficulty walking
• Pain aggravated by standing or walking
• Symptom relief on bending forward
Early diagnosis and appropriate management are essential to prevent neurological deterioration and preserve mobility and quality of life.
Case Report
Patient History
A 62-year-old retired male presented to the orthopedic outpatient department with:
• Chronic lower back pain for 2 years
• Progressive numbness in both lower limbs
• Difficulty walking long distances
• Pain radiating to both legs
• Tingling sensation in feet
• Fatigue while standing
• Progressive reduction in mobility
The patient reported that symptoms worsened during prolonged standing and walking and improved partially while sitting or bending forward.
Over the previous six months, the patient experienced worsening neurogenic claudication, significantly affecting his daily activities and independence.
There was no history of:
• Recent trauma
• Fever
• Bladder or bowel incontinence
• Malignancy
• Tuberculosis
• Previous spinal surgery
Past medical history revealed:
• Hypertension for 8 years
• Osteoarthritis of knees
• Sedentary lifestyle
Clinical Examination
General Examination
• Conscious and oriented
• Pulse rate: 78/min
• Blood pressure: 132/84 mmHg
• Body mass index: 28 kg/m²
• Afebrile
• Hemodynamically stable
Neurological and Spine Examination
Clinical examination revealed:
• Restricted lumbar spine movements
• Lumbar paraspinal muscle tenderness
• Positive shopping cart sign
• Bilateral lower limb paresthesia
• Mild weakness in ankle dorsiflexion
• Reduced walking tolerance
• Decreased deep tendon reflexes in lower limbs
Straight leg raising test was mildly positive bilaterally.
No signs of upper motor neuron lesion were observed.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Lumbar disc prolapse
• Degenerative disc disease
• Peripheral neuropathy
• Cauda equina syndrome
• Vascular claudication
• Lumbar spinal stenosis
The characteristic history of neurogenic claudication with symptom relief on forward flexion strongly suggested lumbar spinal stenosis.
Investigations
Laboratory Findings
• Hemoglobin: Normal
• White blood cell count: Normal
• Blood glucose levels: Mildly elevated
• Renal and liver function tests: Normal
• Inflammatory markers: Within normal limits
Magnetic Resonance Imaging (MRI)
MRI lumbar spine revealed:
• Severe lumbar spinal canal stenosis at L4–L5
• Ligamentum flavum hypertrophy
• Disc bulge causing neural compression
• Bilateral foraminal narrowing
• Compression of traversing nerve roots
The imaging findings confirmed severe degenerative lumbar spinal stenosis.
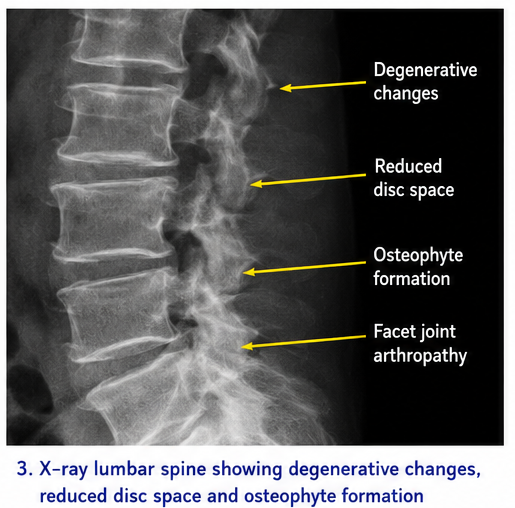
X-Ray Lumbar Spine
Lumbar spine radiography demonstrated:
• Degenerative changes in lumbar vertebrae
• Reduced intervertebral disc space
• Osteophyte formation
• Facet joint arthropathy
Diagnosis
Based on clinical presentation, neurological examination, and MRI findings, a diagnosis of Severe Degenerative Lumbar Spinal Stenosis at L4–L5 with Neurogenic Claudication was established.
Management and Outcome
Initial Conservative Management
The patient was initially advised:
• Activity modification
• Weight reduction
• Physiotherapy
• Postural correction exercises
• Lumbar stabilization exercises
• Analgesics and anti-inflammatory medications
Medical therapy included:
• Nonsteroidal anti-inflammatory drugs (NSAIDs)
• Muscle relaxants
• Neuropathic pain medications
• Calcium and vitamin D supplementation
Physiotherapy
A structured rehabilitation program was initiated including:
• Flexion-based exercises
• Core strengthening
• Gait training
• Stretching exercises
• Supervised ambulation therapy
Despite conservative management for 3 months, symptoms progressively worsened.
Surgical Management
Due to persistent neurological symptoms and reduced functional capacity, the patient underwent:
• Lumbar decompressive laminectomy
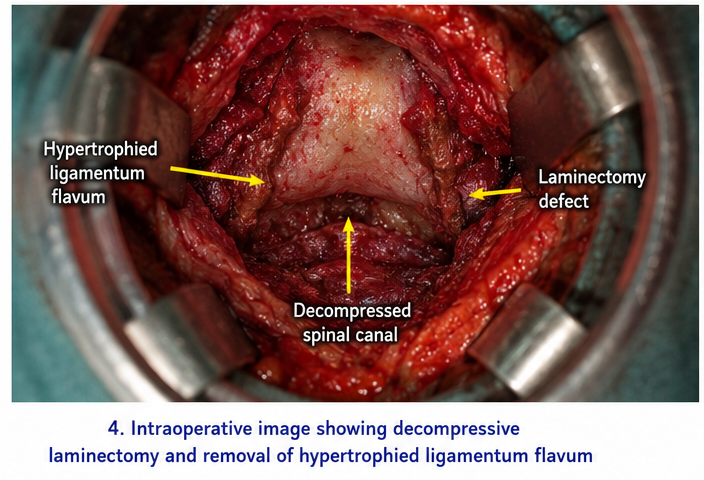
• Removal of hypertrophied ligamentum flavum
• Neural decompression at L4–L5
The procedure was completed successfully without intraoperative complications.
Follow-Up and Clinical Course
At 1 Month
• Significant reduction in lower limb pain
• Improved walking distance
• Reduced numbness and paresthesia
• Better sleep quality
At 3 Months
• Marked improvement in mobility
• Improved lower limb strength
• Significant reduction in neurogenic claudication
• Independent ambulation achieved
At 6 Months
• Stable neurological condition
• Improved quality of life
• No recurrence of severe symptoms
• Continued physiotherapy advised
The patient remained under regular orthopedic follow-up.
Discussion
Pathophysiology
Lumbar spinal stenosis develops primarily due to degenerative changes causing narrowing of the spinal canal and compression of neural structures.
Important pathological mechanisms include:
• Intervertebral disc degeneration
• Osteophyte formation
• Facet joint hypertrophy
• Thickening of ligamentum flavum
• Reduced spinal canal diameter
• Chronic neural compression
• Ischemia of nerve roots
Compression of neural tissues results in pain, sensory disturbances, weakness, and impaired mobility.
Epidemiology
Important epidemiological features include:
• Common in individuals above 50 years
• One of the leading causes of spinal surgery in elderly patients
• Higher prevalence in degenerative spinal disease
• Frequently associated with obesity and sedentary lifestyle
• Significant cause of disability and reduced mobility
The prevalence of lumbar spinal stenosis continues to increase due to aging populations worldwide.
Clinical Manifestations
Common clinical features include:
• Lower back pain
• Neurogenic claudication
• Bilateral leg pain
• Numbness and tingling
• Muscle weakness
• Difficulty standing for prolonged periods
• Reduced walking tolerance
• Postural imbalance
Advanced disease may lead to severe neurological compromise and functional disability.
Diagnostic Considerations
Important diagnostic modalities include:
-
Clinical neurological examination
- X-ray lumbar spine
- MRI spine
- Computed tomography (CT) scan
- Electrophysiological studies
MRI remains the gold standard imaging modality for evaluation of spinal canal narrowing and neural compression.
Treatment Modalities
Conservative Management
Non-surgical treatment options include:
• Physiotherapy
• Weight management
• Activity modification
• Analgesics
• Epidural steroid injections
• Postural rehabilitation
Pharmacological Therapy
Medications commonly used include:
• NSAIDs
• Neuropathic pain agents
• Muscle relaxants
• Corticosteroid injections
Surgical Management
Surgery is considered in:
• Severe stenosis
• Progressive neurological deficits
• Failure of conservative therapy
• Significant mobility impairment
• Severe neurogenic claudication
Common surgical procedures include:
• Laminectomy
• Laminotomy
• Spinal decompression
• Spinal fusion in selected cases
Decompressive surgery remains highly effective in relieving symptoms and improving mobility.
Complications
Potential complications of untreated spinal stenosis include:
• Chronic pain syndrome
• Progressive neurological deficits
• Muscle weakness
• Gait instability
• Falls and fractures
• Reduced mobility
• Psychological distress
• Permanent nerve damage
Delayed intervention may significantly impair quality of life and functional independence.
Prognosis
The prognosis depends upon:
• Severity of spinal narrowing
• Duration of symptoms
• Neurological involvement
• Early diagnosis
• Response to treatment
• Surgical outcomes
• Rehabilitation adherence
Most patients experience substantial symptomatic improvement following timely decompressive surgery and rehabilitation.
Conclusion
Lumbar spinal stenosis is a progressive degenerative spinal disorder that can significantly impair mobility, neurological function, and quality of life if left untreated. Early recognition of neurogenic claudication, lower limb numbness, and chronic back pain is essential for timely diagnosis and intervention.
This case highlights the importance of detailed neurological evaluation, MRI-based diagnosis, individualized conservative therapy, and timely surgical decompression in achieving favorable clinical outcomes. Long-term rehabilitation, lifestyle modification, and regular follow-up remain critical components in the comprehensive management of spinal stenosis.
References
- Katz JN, Harris MB. Lumbar spinal stenosis. https://pubmed.ncbi.nlm.nih.gov/11342813/
- Genevay S, Atlas SJ. Lumbar spinal stenosis. https://pubmed.ncbi.nlm.nih.gov/25844995/
- Kreiner DS, Shaffer WO, Baisden JL, et al. Diagnosis and treatment of degenerative lumbar spinal stenosis. https://pubmed.ncbi.nlm.nih.gov/21160394/
- Ammendolia C, Stuber KJ, Rok E, et al. Nonoperative treatment for lumbar spinal stenosis with neurogenic claudication. https://pubmed.ncbi.nlm.nih.gov/26424350/
- American Academy of Orthopaedic Surgeons. Lumbar Spinal Stenosis. https://orthoinfo.aaos.org/en/diseases--conditions/lumbar-spinal-stenosis/
- National Institute of Arthritis and Musculoskeletal and Skin Diseases. Spinal Stenosis. https://www.niams.nih.gov/health-topics/spinal-stenosis
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Breast Cancer Patients Living Longer Post-Medicaid Expansion
2.
Error on the MGUS-Autoimmune Disease Association.
3.
Patients with chronic myeloid leukemia who take nilotinib are at higher risk for diabetes and hyperlipidemia.
4.
The majority of cancer medications that receive expedited approval end up failing confirmatory trials.
5.
Unified Neuro/Psych Residency Program: New Proposal.
1.
Optimizing Melanoma Treatment: Strategies in Diagnosis, Clinical Research, and Physician Training
2.
Hemoglobin C: Understanding its Role in Sickle Cell Disease
3.
Beyond the Human Eye: How AI Is Redefining Brain Cancer Diagnosis Through Advanced Imaging
4.
Understanding Abemaciclib: A Breakthrough Treatment for Breast Cancer
5.
The Growing Challenge of Haematological Malignancies in Older Adults
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part II
2.
Exploring Potentials of Lorlatinib: The Third Generation ALK-TKI Through CROWN Trial
3.
Molecular Contrast: EGFR Axon 19 vs. Exon 21 Mutations - Part VII
4.
A Conclusive Discussion on CROWN Trial and the Dawn of a New Era in Frontline Management of ALK+ NSCLC
5.
Efficient Management of First line ALK-rearranged NSCLC - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge