Furunculosis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Furunculosis is a common bacterial skin infection involving deep infection of hair follicles, most frequently caused by Staphylococcus aureus. Recurrent furunculosis can significantly impair quality of life and may indicate underlying predisposing factors such as poor hygiene, diabetes mellitus, immunosuppression, obesity, or nasal carriage of pathogenic bacteria. The condition commonly presents with painful erythematous nodules, localized swelling, purulent discharge, and surrounding cellulitis.
We present the case of a 32-year-old male who presented with recurrent painful boils over the neck and axillary region associated with fever, tenderness, and purulent drainage. Clinical examination and microbiological evaluation confirmed furunculosis caused by methicillin-sensitive Staphylococcus aureus (MSSA). The patient was successfully managed with incision and drainage, systemic antibiotics, topical therapy, hygiene counseling, and treatment of predisposing risk factors, resulting in complete clinical recovery without recurrence during follow-up.
This case highlights the importance of early diagnosis, microbiological assessment, adequate drainage, targeted antimicrobial therapy, and preventive hygiene measures in the effective management of furunculosis.
Introduction
Furunculosis is a deep follicular infection characterized by painful inflammatory nodules involving hair follicles and surrounding subcutaneous tissue. These lesions, commonly known as boils, usually develop following bacterial invasion of hair follicles, most frequently by Staphylococcus aureus. Multiple interconnected furuncles may coalesce to form carbuncles, resulting in deeper tissue involvement and systemic manifestations.
The condition commonly affects areas subjected to friction, perspiration, and hair growth such as the neck, axillae, buttocks, thighs, and face. Recurrent furunculosis remains an important dermatological concern because of repeated infections, discomfort, cosmetic issues, and risk of complications including cellulitis and abscess formation.
Several predisposing factors contribute to furunculosis, including:
• Poor personal hygiene
• Diabetes mellitus
• Obesity
• Immunosuppression
• Nasal carriage of Staphylococcus aureus
• Excessive sweating
• Friction from tight clothing
• Malnutrition
• Chronic skin diseases
• Recurrent skin trauma
Common clinical manifestations include:
• Painful erythematous nodules
• Localized swelling
• Tenderness
• Pus discharge
• Fever
• Surrounding cellulitis
• Fatigue
• Recurrent lesions
• Regional lymphadenopathy
Early diagnosis and appropriate antimicrobial management are essential to prevent complications and recurrence.
Case Report
Patient History
A 32-year-old male presented to the dermatology outpatient department with:
• Multiple painful boils over the posterior neck and both axillae
• Progressive swelling for 7 days
• Purulent discharge from one lesion
• Fever and malaise
• Difficulty in neck movement due to pain
• Local warmth and tenderness
The patient reported recurrent similar lesions over the previous six months with temporary improvement following local treatment.
Past medical history revealed:
• Poorly controlled type 2 diabetes mellitus
• Obesity
• Excessive sweating during work
• Frequent skin friction from tight clothing
There was no history of:
• Tuberculosis
• HIV infection
• Intravenous drug abuse
• Chronic steroid use
• Previous hospitalization
Clinical Examination
General Examination
Clinical examination revealed:
• Conscious and oriented patient
• Mild fever
• Pulse rate: 92/min
• Blood pressure: 128/82 mmHg
• Mild dehydration
• Body mass index suggestive of obesity
Local Examination
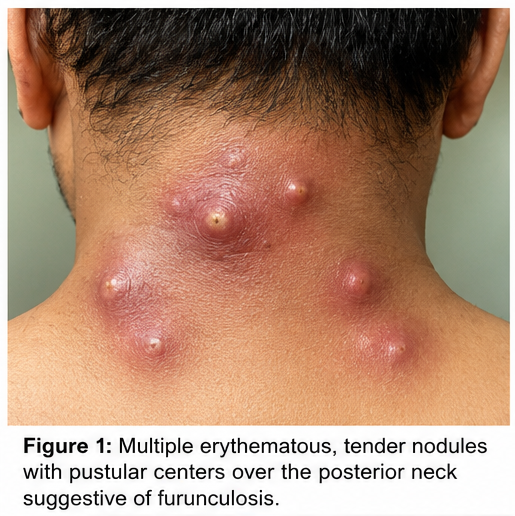
Dermatological examination demonstrated:
• Multiple erythematous tender nodules over the neck and axillae
• Central pustular points in some lesions
• One fluctuant lesion with purulent discharge
• Surrounding induration and cellulitis
• Local warmth and tenderness
• No evidence of necrotizing infection
Regional lymph nodes were mildly enlarged and tender.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Furunculosis
• Carbuncle
• Hidradenitis suppurativa
• Infected epidermoid cyst
• Cutaneous abscess
• Folliculitis
• Cellulitis
The recurrent painful nodules with purulent discharge strongly suggested furunculosis.
Investigations
Laboratory Findings
Initial laboratory investigations revealed:
• Mild leukocytosis
• Elevated ESR and CRP
• Elevated fasting blood glucose
• HbA1c: Elevated
• Renal and liver function tests: Within normal limits
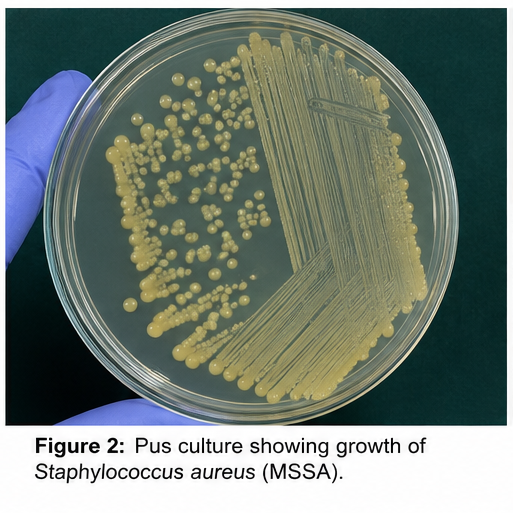
Microbiological Evaluation
Pus culture demonstrated:
• Growth of methicillin-sensitive Staphylococcus aureus (MSSA)
Antibiotic sensitivity testing showed susceptibility to:
• Clindamycin
• Amoxicillin-clavulanate
• Doxycycline
Additional Evaluation
Further investigations revealed:
• HIV serology: Negative
• No evidence of systemic immunosuppression
Diagnosis
Based on clinical presentation, recurrent painful boils, microbiological findings, and associated risk factors, a diagnosis of Recurrent Furunculosis secondary to Staphylococcus aureus infection was established.
Management and Outcome
Initial Medical Management
The patient underwent:
• Incision and drainage of fluctuant lesions

• Sterile wound dressing
• Local antiseptic cleansing
• Warm compress application
Systemic antibiotic therapy was initiated with:
• Oral clindamycin
Additional management included:
• Blood glucose optimization
• Pain management
• Hydration
• Hygiene counseling
The patient was advised:
• Regular bathing with antiseptic soap
• Avoidance of tight clothing
• Proper drying of skin folds
• Avoid sharing towels and personal items
• Weight reduction measures
Follow-Up and Clinical Course
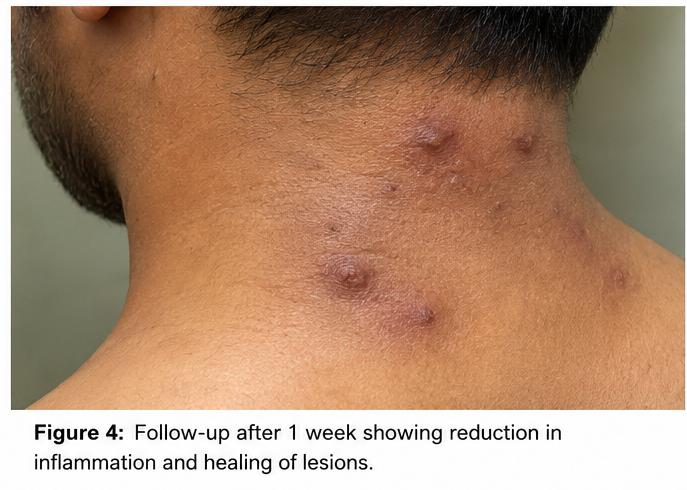
At 1 Week
• Reduction in pain and swelling
• Decreased purulent discharge
• Improvement in fever
• Better neck mobility
At 3 Weeks
• Significant healing of lesions
• Resolution of cellulitis
• No new boils observed
• Improved glycemic control
At 2 Months
• Complete healing with minimal scarring
• No recurrence of furuncles
• Improved hygiene practices
• Better diabetic control

The patient remained under regular dermatology follow-up.
Discussion
Pathophysiology
Furunculosis develops due to bacterial invasion of hair follicles leading to deep follicular inflammation and abscess formation. Staphylococcus aureus produces toxins and inflammatory mediators that contribute to tissue destruction and pus formation.
Important pathological mechanisms include:
• Hair follicle infection
• Neutrophilic inflammation
• Local tissue necrosis
• Abscess formation
• Surrounding cellulitis
• Recurrent bacterial colonization
Persistent bacterial carriage and uncontrolled risk factors contribute to recurrent disease.
Epidemiology
Important epidemiological features include:
• Common bacterial skin infection worldwide
• Frequently affects adolescents and adults
• Higher prevalence in diabetic and immunocompromised individuals
• Increased incidence in crowded environments
• Associated with poor hygiene and excessive sweating
• Commonly caused by Staphylococcus aureus
Recurrent furunculosis contributes substantially to healthcare burden and reduced quality of life.
Clinical Manifestations
Clinical presentation varies according to severity and extent of infection.
Common manifestations include:
• Painful boils
• Erythema
• Swelling
• Purulent discharge
• Fever
• Tenderness
• Cellulitis
• Regional lymphadenopathy
• Recurrent lesions
Large carbuncles may produce significant systemic symptoms.
Diagnostic Considerations
Important diagnostic modalities include:
- Clinical examination
- Pus culture and sensitivity
- Blood glucose evaluation
- Complete blood count
- Inflammatory markers
- Screening for immunosuppression
Microbiological testing helps guide appropriate antimicrobial therapy and identify resistant organisms.
Treatment Modalities
Supportive Management
Supportive care includes:
• Warm compresses
• Local wound care
• Hygiene maintenance
• Glycemic control
• Pain management
Pharmacological Therapy
Commonly used antibiotics include:
• Clindamycin
• Doxycycline
• Amoxicillin-clavulanate
• Trimethoprim-sulfamethoxazole
Severe infections may require intravenous antibiotics and hospitalization.
Surgical Management
Incision and drainage remain essential for fluctuant abscesses and larger lesions.
Preventive Measures
Preventive strategies include:
• Regular personal hygiene
• Glycemic control
• Weight management
• Avoidance of skin trauma
• Proper wound care
• Avoidance of sharing personal items
• Nasal decolonization in recurrent cases
Early treatment significantly reduces recurrence and complications.
Complications
Potential complications include:
• Cellulitis
• Carbuncle formation
• Abscess extension
• Scarring
• Recurrent infection
• Sepsis
• Chronic skin damage
Delayed treatment may increase morbidity and recurrence risk.
Prognosis
The prognosis depends upon:
• Early diagnosis
• Appropriate antibiotic therapy
• Adequate drainage
• Glycemic control
• Hygiene maintenance
• Prevention of recurrence
• Immune status
Most patients achieve complete recovery with timely treatment and correction of underlying risk factors.
Conclusion
Furunculosis is a common yet potentially recurrent bacterial skin infection that can cause significant discomfort and complications if inadequately treated. Early recognition of painful inflammatory nodules, microbiological confirmation, incision and drainage, targeted antimicrobial therapy, and correction of predisposing factors are essential for successful management.
This case highlights the importance of hygiene measures, diabetes control, patient counseling, and appropriate follow-up in preventing recurrence and achieving favorable clinical outcomes in furunculosis.
References
- World Health Organization. Skin and soft tissue infections. https://www.who.int/
- Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections. https://pubmed.ncbi.nlm.nih.gov/24947530/
- Centers for Disease Control and Prevention. Staphylococcus aureus Skin Infections. https://www.cdc.gov/mrsa/community/index.html
- Miller LG, Cho J, Crespo HJ. Management of recurrent furunculosis and community-associated staphylococcal infections. https://pubmed.ncbi.nlm.nih.gov/22763663/
- Lo WT, Wang CC. Recurrent furunculosis caused by Staphylococcus aureus: Epidemiology and treatment strategies. https://pubmed.ncbi.nlm.nih.gov/19389024/
- May AK, Stafford RE, Bulger EM, et al. Treatment of complicated skin and soft tissue infections. https://pubmed.ncbi.nlm.nih.gov/24247125/
- DermNet NZ. Furuncle and Carbuncle Overview. https://dermnetnz.org/topics/boil-and-carbuncle
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge