Intraocular Foreign Body Following High-Velocity Metallic Ocular Trauma Successfully Managed with Pars Plana Vitrectomy – A Case Report
OthersPage Navigation
Abstract
Intraocular foreign body (IOFB) is a vision-threatening ocular emergency that commonly results from high-velocity penetrating eye injuries sustained during industrial, construction, or agricultural activities. Metallic foreign bodies account for the majority of IOFBs and frequently occur in young working males who fail to use appropriate protective eyewear. Delayed diagnosis or management may lead to severe complications including endophthalmitis, retinal detachment, vitreous hemorrhage, proliferative vitreoretinopathy, siderosis bulbi, traumatic cataract, and permanent visual loss. Prompt diagnosis using detailed ophthalmic examination and orbital imaging, followed by timely surgical intervention, plays a critical role in preserving vision.
We report the case of a 29-year-old metal factory worker who presented with sudden pain, redness, watering, blurred vision, and photophobia in his right eye after sustaining a high-velocity metallic injury while hammering steel without protective goggles. Slit-lamp examination revealed a self-sealed corneal entry wound with traumatic cataract. Computed tomography (CT) of the orbit confirmed a retained metallic intraocular foreign body lodged within the vitreous cavity. The patient underwent pars plana vitrectomy with successful removal of the foreign body, intravitreal antibiotics, and retinal laser photocoagulation. Vision improved remarkably during follow-up without significant complications. This case emphasizes the importance of early diagnosis, prompt surgical management, and preventive eye protection in reducing visual morbidity associated with intraocular foreign bodies.
Introduction
Intraocular foreign body refers to any external object retained within the globe following penetrating ocular trauma. IOFBs constitute approximately 18–41% of all open-globe injuries and represent one of the leading causes of unilateral visual impairment among young adults. Metallic fragments generated during grinding, drilling, hammering, welding, and industrial machining are the most common causative agents.
Risk factors include:
- Metal grinding and hammering
- Welding activities
- Construction work
- Agricultural injuries
- Lack of protective eyewear
- High-speed projectile injuries
Patients may present with:
- Sudden ocular pain
- Blurred vision
- Redness
- Watering
- Photophobia
- Foreign body sensation
- Decreased visual acuity
Potential complications include traumatic cataract, vitreous hemorrhage, retinal tears, retinal detachment, endophthalmitis, siderosis bulbi, glaucoma, and irreversible blindness. Early surgical intervention significantly improves visual prognosis.
Case Report
Patient History
A 29-year-old man presented to the emergency ophthalmology department with severe pain, redness, watering, and sudden diminution of vision in the right eye for six hours. The symptoms developed immediately after a metallic fragment struck his eye while hammering steel at work. The patient admitted that he was not wearing protective safety goggles.
There was no history of previous ocular trauma, ocular surgery, diabetes mellitus, hypertension, or systemic illness.
Clinical Examination
General examination was unremarkable.
Vital signs were stable:
- Pulse rate: 82 beats/minute
- Blood pressure: 122/76 mmHg
- Respiratory rate: 18 breaths/minute
- Temperature: Afebrile
Ophthalmic examination revealed:
Right eye
- Visual acuity: Counting fingers at 2 meters
- Circumcorneal congestion
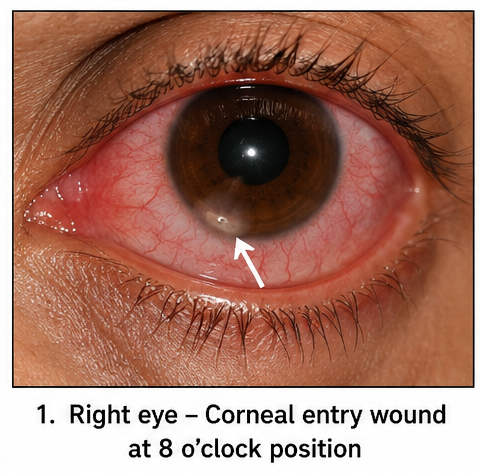
- Small self-sealed corneal entry wound
- Mild anterior chamber reaction
- Traumatic cataract
- Positive Seidel test absent
- Relative afferent pupillary defect absent
Left eye
- Visual acuity: 6/6
- Normal anterior and posterior segments
Fundus examination of the injured eye was limited because of traumatic cataract.
Differential Diagnosis
The following conditions were considered:
- Retained intraocular foreign body
- Open globe injury
- Corneal foreign body
- Traumatic cataract
- Globe perforation
- Vitreous hemorrhage
- Retinal detachment
Investigations
Laboratory Evaluation
Routine laboratory investigations were within normal limits.
- Hemoglobin: 13.6 g/dL
- Total leukocyte count: 7,900/mm³
- Platelet count: 265,000/mm³
- Blood glucose: Normal
Slit-Lamp Examination
Slit-lamp biomicroscopy demonstrated:
- Full-thickness corneal entry wound
- Mild anterior chamber inflammation
- Traumatic cataract
- No iris prolapse
CT Orbit
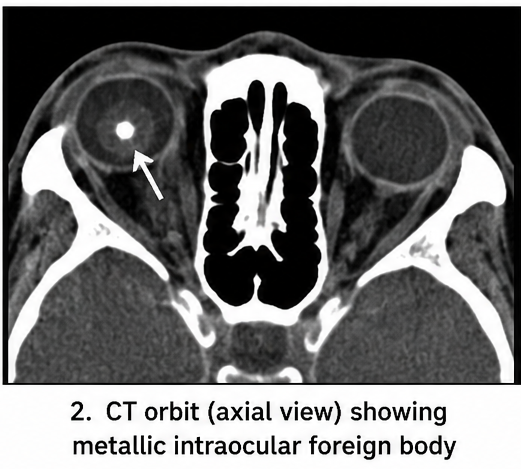
Non-contrast CT orbit revealed:
- Hyperdense metallic foreign body measuring approximately 3 mm
- Foreign body located within the posterior vitreous cavity
- Intact globe contour
- No orbital fractures
- No intraorbital hemorrhage
B-scan ultrasonography demonstrated mild vitreous echoes without retinal detachment.
Diagnosis
Based on the history, clinical findings, slit-lamp examination, and CT imaging, a diagnosis of penetrating open-globe injury with retained metallic intraocular foreign body involving the vitreous cavity was established.
Management and Outcome
The patient received immediate tetanus prophylaxis and was started on:
- Intravenous broad-spectrum antibiotics
- Topical moxifloxacin eye drops
- Cycloplegic eye drops
- Analgesics
- Protective eye shield
Within 24 hours, the patient underwent 23-gauge pars plana vitrectomy under general anesthesia.
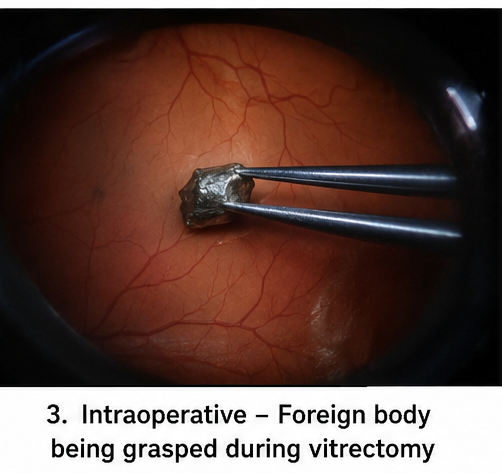
Intraoperative findings included:
- Metallic foreign body within the vitreous cavity
- Localized vitreous hemorrhage
- Small retinal impact site
- No retinal detachment
The foreign body was removed using intraocular forceps through an enlarged sclerotomy.
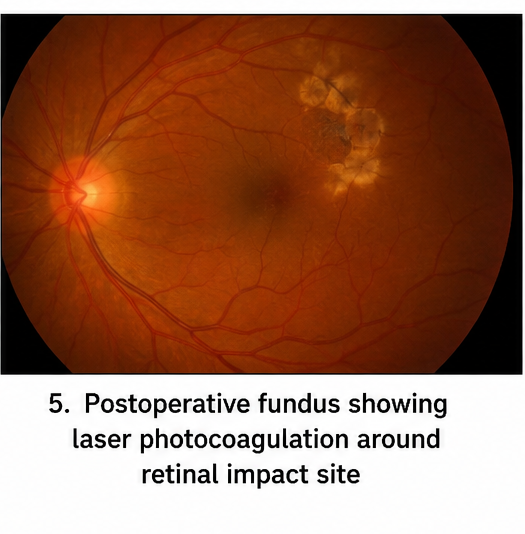
Complete vitrectomy was performed, followed by endolaser photocoagulation around the retinal impact site. Intravitreal vancomycin and ceftazidime were administered prophylactically to reduce the risk of endophthalmitis. The traumatic cataract was planned for secondary management after adequate healing.

The postoperative period remained uneventful.
Follow-Up
One Week
- Pain completely resolved
- Corneal wound healed well
- Mild postoperative inflammation
- Retina attached
One Month
- Best corrected visual acuity improved to 6/18
- No evidence of infection
- Stable retinal laser scars
- Resolution of vitreous hemorrhage
Three Months
Following cataract surgery with intraocular lens implantation, best corrected visual acuity improved to 6/9. Fundus examination demonstrated an attached retina with no evidence of retinal detachment, siderosis bulbi, or proliferative vitreoretinopathy. The patient resumed routine occupational activities with advice regarding mandatory eye protection.
Discussion
Retained intraocular foreign bodies are ophthalmic emergencies requiring immediate diagnosis and multidisciplinary management. Metallic foreign bodies are responsible for nearly 80–90% of IOFB injuries and typically affect young men employed in industrial occupations. Most injuries occur during hammering, grinding, drilling, and welding, particularly when protective eyewear is not used.
Clinical presentation depends on the size, composition, velocity, and location of the foreign body. Small self-sealed corneal wounds may initially appear deceptively benign despite significant intraocular damage. Careful history taking, slit-lamp examination, dilated fundus examination, and orbital CT scanning remain essential for diagnosis. CT orbit is considered the imaging modality of choice because of its high sensitivity for detecting metallic IOFBs. MRI should be avoided when metallic foreign bodies are suspected.
Early surgical removal minimizes the risks of infectious endophthalmitis, retinal detachment, toxic siderosis bulbi, and chronic inflammation. Pars plana vitrectomy has become the standard surgical technique for posterior segment IOFBs, allowing removal of the foreign body, clearance of vitreous hemorrhage, treatment of retinal tears, and prevention of tractional complications. Prophylactic intravitreal antibiotics are commonly administered in high-risk injuries to reduce postoperative infection.
Visual prognosis depends on several factors including presenting visual acuity, size and composition of the foreign body, associated retinal injury, presence of endophthalmitis, and timing of surgical intervention. Patients treated within the first 24 hours generally achieve better visual outcomes than those with delayed presentation. Prevention remains equally important, as consistent use of certified protective eyewear can substantially reduce the incidence of occupational ocular trauma.
Prognosis
The prognosis of intraocular foreign body injuries depends on early recognition, prompt imaging, and timely surgical intervention. Patients without retinal detachment or endophthalmitis generally experience favorable visual recovery following pars plana vitrectomy. Delayed diagnosis increases the risk of irreversible complications including retinal detachment, siderosis bulbi, proliferative vitreoretinopathy, chronic uveitis, and permanent blindness. Long-term follow-up is recommended to monitor retinal integrity, intraocular pressure, and late complications. Occupational safety education and the routine use of protective eye shields remain the most effective preventive strategies.
Conclusion
Intraocular foreign body is a true ophthalmic emergency requiring rapid diagnosis and prompt surgical management to preserve vision. High clinical suspicion should be maintained in all patients presenting with high-velocity ocular injuries, even when external wounds appear minimal. CT imaging plays a pivotal role in diagnosis, while pars plana vitrectomy enables safe removal of posterior segment foreign bodies and management of associated retinal injuries. Early intervention, appropriate antimicrobial therapy, and meticulous postoperative follow-up contribute significantly to favorable visual outcomes. Preventive measures, particularly the routine use of protective eyewear in industrial settings, remain essential for reducing the burden of vision-threatening ocular trauma.
References
- Loporchio D, Mukkamala L, Gorukanti K, et al. Intraocular Foreign Bodies: A Review. Survey of Ophthalmology. 2016;61(5):582–596. https://pubmed.ncbi.nlm.nih.gov/26997432/
- American Academy of Ophthalmology. Open Globe Injury: Assessment and Preoperative Management. EyeWiki. https://eyewiki.aao.org/Open_Globe_Injury
- Zhang Y, Zhang M, Jiang C, Qiu HY. Intraocular foreign bodies in China: clinical characteristics and prognostic factors. BMC Ophthalmology. 2011;11:28. https://pubmed.ncbi.nlm.nih.gov/22029815/
- Colyer MH, Chun DW, Bower KS, Dick JS, Weichel ED. Perforating globe injuries during modern warfare. Ophthalmology. 2008;115(11):2087–2093. https://pubmed.ncbi.nlm.nih.gov/18538402
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge