Cardiomegaly: Progressive Cardiac Enlargement Associated with Hypertensive Heart Disease – A Case Report
OthersPage Navigation
Abstract
Cardiomegaly refers to abnormal enlargement of the heart and is often an indicator of underlying cardiovascular pathology rather than a disease itself. It commonly results from chronic hypertension, valvular heart disease, cardiomyopathy, ischemic heart disease, or congenital cardiac abnormalities. Progressive cardiac enlargement may eventually lead to heart failure, arrhythmias, thromboembolic complications, and increased mortality if left untreated.
We present the case of a 58-year-old male who presented with progressive exertional dyspnea, lower extremity edema, and fatigue. Chest radiography demonstrated an enlarged cardiac silhouette, while echocardiography revealed left ventricular hypertrophy and dilatation with reduced systolic function. Further evaluation established hypertensive heart disease as the primary etiology. The patient was managed with antihypertensive therapy, diuretics, and lifestyle modification, resulting in symptomatic improvement and stabilization of cardiac function.
This case highlights the importance of early recognition of cardiomegaly, comprehensive cardiovascular evaluation, and timely intervention to prevent progression to advanced heart failure.
Introduction
Cardiomegaly is defined as enlargement of the heart beyond normal anatomical dimensions. It may involve enlargement of one or more cardiac chambers and frequently reflects chronic structural or functional cardiac stress.
The condition is commonly identified through chest radiography, where an increased cardiothoracic ratio suggests cardiac enlargement. However, echocardiography remains the gold standard for evaluating chamber size, ventricular function, and associated structural abnormalities.
Common causes of cardiomegaly include:
• Chronic hypertension
• Coronary artery disease
• Dilated cardiomyopathy
• Valvular heart disease
• Congenital heart disorders
• Arrhythmias
• Pulmonary hypertension
Clinical manifestations vary depending on the severity and underlying cause but commonly include dyspnea, fatigue, exercise intolerance, edema, and palpitations.
Early diagnosis and management are essential to prevent irreversible myocardial damage and cardiovascular complications.
Case Report
Patient History
A 58-year-old male presented to the cardiology outpatient department with complaints of:
• Progressive shortness of breath for eight months
• Fatigue during routine activities
• Swelling of both ankles for three months
• Occasional palpitations
• Reduced exercise tolerance
The symptoms had gradually worsened over the preceding six months.
The patient denied chest pain, syncope, fever, or recent respiratory infections.
Past medical history revealed:
• Hypertension for 15 years
• Type 2 diabetes mellitus for 8 years
• Dyslipidemia
Medication adherence was irregular, and blood pressure control had been suboptimal for several years.
Family history was significant for hypertension and ischemic heart disease.
Clinical Examination
General Examination
The patient appeared mildly dyspneic at rest.
Vital signs were as follows:
• Blood pressure: 168/96 mmHg
• Pulse rate: 92 beats/minute
• Respiratory rate: 22 breaths/minute
• Temperature: Afebrile
• Oxygen saturation: 96% on room air
Physical examination revealed:
• Bilateral pitting pedal edema
• Elevated jugular venous pressure
• Mild peripheral cyanosis
Cardiovascular Examination
Cardiac examination demonstrated:
• Laterally displaced apical impulse
• Presence of S3 gallop rhythm
• Mild systolic murmur at the apex
• Regular heart rhythm
Respiratory Examination
Findings included:
• Bibasal fine crepitations
• Reduced air entry at lower lung zones
These findings suggested early congestive heart failure.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Hypertensive heart disease
• Dilated cardiomyopathy
• Ischemic cardiomyopathy
• Valvular heart disease
• Pericardial effusion
• Congestive heart failure
Because of the long-standing history of uncontrolled hypertension, hypertensive cardiomyopathy was strongly suspected.
Investigations
Laboratory Evaluation
Complete blood count was normal.
Biochemical investigations revealed:
• Fasting blood glucose: 162 mg/dL
• HbA1c: 8.1%
• Total cholesterol: 242 mg/dL
• LDL cholesterol: 164 mg/dL
• Serum creatinine: 1.1 mg/dL
• Sodium: 138 mEq/L
• Potassium: 4.4 mEq/LChest Radiography
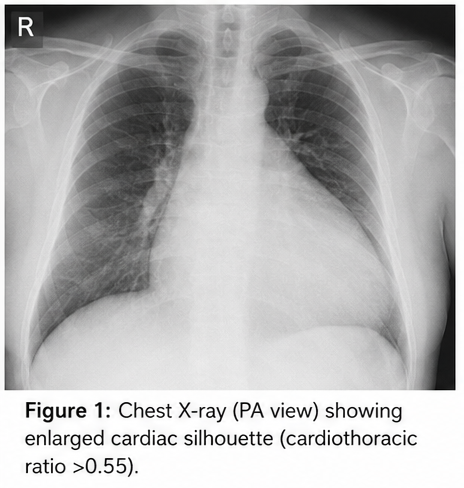
Posteroanterior chest X-ray revealed:
• Markedly enlarged cardiac silhouette
• Cardiothoracic ratio greater than 0.55
• Mild pulmonary vascular congestion
These findings were consistent with cardiomegaly.
Electrocardiography
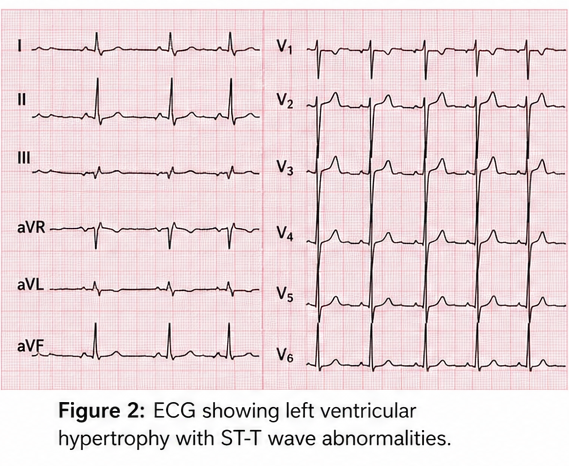
Electrocardiogram demonstrated:
• Left ventricular hypertrophy
• Left axis deviation
• Nonspecific ST-T wave abnormalities
• Sinus rhythm
Transthoracic Echocardiography
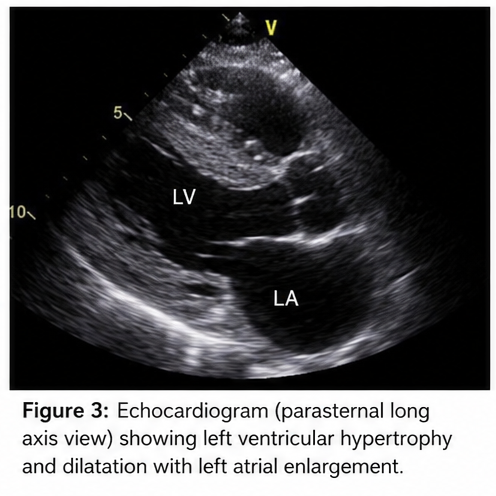
Echocardiography demonstrated:
• Left ventricular hypertrophy
• Left ventricular dilatation
• Ejection fraction of 40%
• Mild mitral regurgitation
• Left atrial enlargement
• Grade II diastolic dysfunction
No significant pericardial effusion was noted.
Cardiac Magnetic Resonance Imaging
Cardiac MRI further confirmed:
• Enlarged left ventricular chamber
• Increased myocardial mass
• Absence of infiltrative cardiomyopathy
• No evidence of myocardial scar formation
Biomarker Assessment
Brain Natriuretic Peptide (BNP) level was elevated at 420 pg/mL, supporting the diagnosis of heart failure.
Diagnosis
Based on clinical findings, imaging studies, and cardiovascular evaluation, a diagnosis of: Cardiomegaly Secondary to Hypertensive Heart Disease with Early Congestive Heart Failure was established.
Management and Outcome
Initial Management
The patient was admitted for stabilization and optimization of medical therapy.
Treatment included:
• Intravenous loop diuretics
• Angiotensin-converting enzyme inhibitor
• Beta-blocker therapy
• Mineralocorticoid receptor antagonist
• Statin therapy
• Strict blood pressure control
Lifestyle interventions included:
• Sodium restriction
• Weight reduction
• Smoking cessation counseling
• Structured physical activity program
• Diabetic control optimization
Hospital Course
During hospitalization, the patient demonstrated:
• Improved breathing
• Reduction in lower limb edema
• Improved exercise tolerance

Blood pressure gradually improved to 132/80 mmHg.
No arrhythmias were observed during monitoring.
Follow-Up
At 1 Month
Clinical improvement included:
• Significant reduction in dyspnea
• Resolution of ankle edema
• Better exercise capacity
Blood pressure remained controlled.
At 3 Months
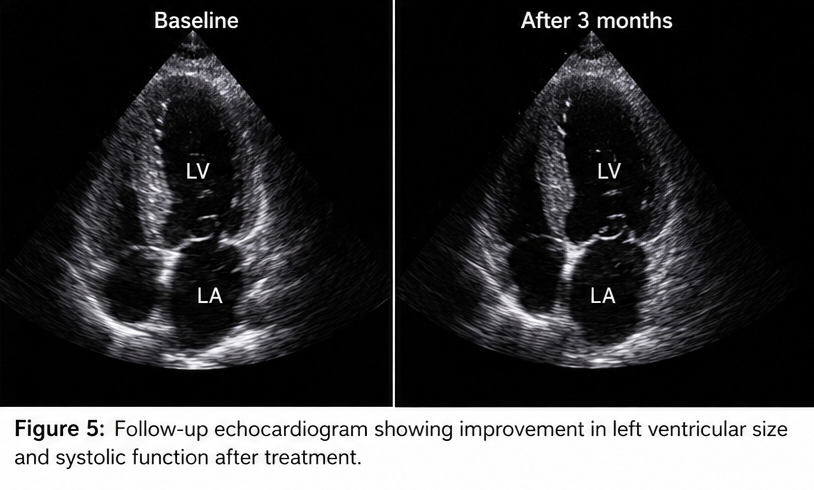
Repeat echocardiography demonstrated:
• Mild reduction in left ventricular dimensions
• Improved systolic function
• Ejection fraction increased to 45%
The patient reported improved quality of life and ability to perform daily activities.
At 12 Months
Long-term follow-up showed:
• Stable cardiac function
• Controlled hypertension
• No hospitalization for heart failure
• Sustained symptom improvement
The patient remained compliant with medications and lifestyle modifications.
Discussion
Pathophysiology
Cardiomegaly develops when the myocardium undergoes adaptive structural changes in response to chronic hemodynamic stress.
In hypertension, prolonged pressure overload leads to:
• Myocardial hypertrophy
• Increased ventricular wall thickness
• Progressive chamber enlargement
• Reduced ventricular compliance
Over time, compensatory mechanisms become insufficient, resulting in ventricular dysfunction and heart failure.
Neurohormonal activation involving:
• Renin-angiotensin-aldosterone system
• Sympathetic nervous system
• Inflammatory mediators
contributes significantly to disease progression.
Clinical Features
Symptoms vary depending on disease severity and underlying etiology.
Common manifestations include:
• Dyspnea on exertion
• Orthopnea
• Fatigue
• Peripheral edema
• Reduced exercise capacity
• Palpitations
• Chest discomfort
Advanced disease may lead to:
• Pulmonary edema
• Arrhythmias
• Cardiogenic shock
• Sudden cardiac death
Differential Diagnosis
Dilated Cardiomyopathy
Typically presents with marked ventricular dilation and reduced systolic function without a primary hypertensive cause.
Ischemic Cardiomyopathy
Associated with coronary artery disease and prior myocardial infarction.
Valvular Heart Disease
Valve abnormalities may cause secondary chamber enlargement and heart failure.
Pericardial Effusion
Can mimic cardiomegaly on chest radiographs but is distinguishable through echocardiography.
Congenital Heart Disease
May produce cardiac enlargement due to chronic volume overload.
Treatment Options
Management focuses on addressing the underlying cause and preventing progression.
Medical Therapy
Includes:
• ACE inhibitors or ARBs
• Beta-blockers
• Diuretics
• Mineralocorticoid receptor antagonists
• SGLT2 inhibitors when appropriate
• Lipid-lowering agents
Lifestyle Modification
Important measures include:
• Blood pressure control
• Dietary sodium restriction
• Weight management
• Regular physical activity
• Smoking cessation
Advanced Therapies
Severe cases may require:
• Cardiac resynchronization therapy
• Implantable cardioverter-defibrillator
• Ventricular assist devices
• Heart transplantation
Complications
Potential complications include:
• Chronic heart failure
• Atrial fibrillation
• Ventricular arrhythmias
• Stroke
• Thromboembolism
• Sudden cardiac death
• Progressive ventricular dysfunction
Early intervention significantly reduces the risk of these adverse outcomes.
Prognosis
The prognosis depends on:
• Underlying etiology
• Degree of ventricular dysfunction
• Timeliness of diagnosis
• Blood pressure control
• Treatment adherence
Patients diagnosed early and managed appropriately often achieve substantial symptom improvement and long-term stabilization.
Advances in cardiovascular imaging, pharmacotherapy, and heart failure management continue to improve patient outcomes.
Conclusion
Cardiomegaly is an important clinical indicator of underlying cardiovascular disease and may represent a precursor to heart failure if left untreated. This case demonstrates the impact of chronic uncontrolled hypertension on cardiac structure and function. Comprehensive diagnostic evaluation, including imaging and functional assessment, is essential for determining the underlying cause. Early initiation of evidence-based medical therapy and aggressive risk-factor modification can significantly improve symptoms, prevent disease progression, and enhance quality of life. Long-term follow-up remains critical for monitoring cardiac function and reducing cardiovascular morbidity and mortality.
References
- Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the Guideline for the Management of Heart Failure. Circulation. 2017;136:e137-e161. PubMed: https://pubmed.ncbi.nlm.nih.gov/28455343/
- Messerli FH, Rimoldi SF, Bangalore S. The transition from hypertension to heart failure: contemporary update. Journal of the American College of Cardiology. 2017;69(24):3042-3054. PubMed: https://pubmed.ncbi.nlm.nih.gov/28641795/
- Maron BJ, Towbin JA, Thiene G, et al. Contemporary definitions and classification of cardiomyopathies. Circulation. 2006;113(14):1807-1816. PubMed: https://pubmed.ncbi.nlm.nih.gov/16567565/
- Bozkurt B, Coats AJS, Tsutsui H, et al. Universal Definition and Classification of Heart Failure. Journal of Cardiac Failure. 2021;27(4):387-413. PubMed: https://pubmed.ncbi.nlm.nih.gov/33663906/
- Groenewegen A, Rutten FH, Mosterd A, Hoes AW. Epidemiology of heart failure. European Journal of Heart Failure. 2020;22(8):1342-1356. PubMed: https://pubmed.ncbi.nlm.nih.gov/32483830/
- Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults. European Heart Journal Cardiovascular Imaging. 2015;16(3):233-270. PubMed: https://pubmed.ncbi.nlm.nih.gov/25712077
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge