Contact Dermatitis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcome – A Case Report
OthersPage Navigation
Abstract
Contact dermatitis is a common inflammatory skin disorder resulting from direct exposure to irritants or allergens that trigger cutaneous inflammation. It is characterized by erythema, pruritus, edema, vesiculation, scaling, and skin barrier dysfunction. The condition may significantly impair quality of life and occupational productivity, particularly when recurrent or chronic. Although contact dermatitis is generally benign, delayed diagnosis and continued exposure to causative agents may lead to chronic eczema, secondary infection, and persistent skin damage.
We present the case of a 35-year-old female who developed progressive itching, erythema, and scaling over both hands following repeated exposure to household cleaning products. Clinical evaluation, exposure history, dermatological examination, and patch testing confirmed allergic contact dermatitis. The patient was successfully treated with allergen avoidance, topical corticosteroids, emollient therapy, and patient education, resulting in complete clinical recovery.
This case highlights the importance of detailed exposure history, accurate diagnosis, patch testing, and preventive strategies in achieving favorable outcomes in patients with contact dermatitis.
Introduction
Contact dermatitis is an inflammatory skin disease caused by exposure to exogenous substances that either directly damage the skin barrier or induce a delayed hypersensitivity reaction. It is one of the most common dermatological conditions encountered in both primary care and specialist practice.
The condition is broadly classified into:
• Irritant Contact Dermatitis (ICD)
• Allergic Contact Dermatitis (ACD)
Irritant contact dermatitis results from direct chemical or physical injury to the skin, whereas allergic contact dermatitis is a T-cell-mediated delayed hypersensitivity reaction that develops after sensitization to an allergen.
Predisposing factors include:
• Frequent hand washing
• Occupational chemical exposure
• Household cleaning products
• Cosmetic products
• Metal exposure
• Rubber products
• Preservatives and fragrances
• Atopic skin conditions
Clinical manifestations range from mild erythema and itching to severe vesiculation, fissuring, and chronic lichenification. Accurate diagnosis and early intervention are essential to prevent chronic disease and recurrence.
Case Report
Patient History
A 35-year-old female presented to the dermatology outpatient department with complaints of:
• Intense itching over both hands for 3 weeks
• Redness of the skin
• Dryness and scaling
• Burning sensation after cleaning activities
• Painful skin cracks near the finger joints
The symptoms had gradually worsened despite the use of over-the-counter moisturizers.
The patient reported daily exposure to household cleaning agents and detergents without using protective gloves.

The patient denied:
• Fever
• Joint pain
• Oral ulcers
• Drug allergies
• Recent infections
• Previous dermatological disorders
Past medical history was unremarkable.
There was no family history of psoriasis, eczema, or autoimmune disease.
Clinical Examination
General Examination
• Blood pressure: 118/76 mmHg
• Pulse rate: 82/min
• Respiratory rate: 16/min
• Temperature: 98.4°F
• Oxygen saturation: 99% on room air
The patient appeared comfortable and clinically stable.
Dermatological Examination
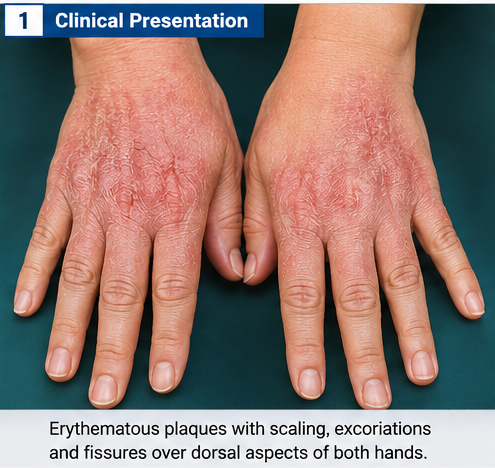
Examination of both hands revealed:
• Well-defined erythematous plaques
• Fine scaling
• Excoriation marks
• Mild edema
• Superficial fissures
• Dry and rough skin texture
• No purulent discharge
• No evidence of secondary infection
The lesions were predominantly distributed over the dorsal surfaces of both hands and fingers.
Nails and mucosal surfaces appeared normal.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Allergic contact dermatitis
• Irritant contact dermatitis
• Atopic dermatitis
• Psoriasis
• Tinea manuum
• Dyshidrotic eczema
The temporal relationship between cleaning product exposure and symptom exacerbation strongly suggested contact dermatitis.
Investigations
Laboratory Evaluation
Routine investigations revealed:
• Hemoglobin: 12.9 g/dL
• Total leukocyte count: 8,400/mm³
• Platelet count: 276,000/mm³
• ESR: 18 mm/hr
• CRP: 4 mg/L
Laboratory parameters were within normal limits.
KOH Examination
Skin scrapings were examined for fungal infection.
Results showed:
• No fungal hyphae
• No dermatophyte infection
Patch Testing
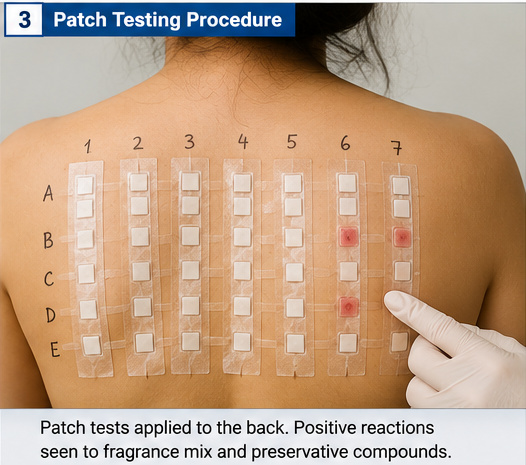
Patch testing was performed using a standard allergen panel.
Results demonstrated:
• Positive reaction to fragrance mix
• Positive reaction to preservative compounds
• Delayed hypersensitivity response at 48 hours
• Persistent positivity at 72 hours
Dermoscopy
Dermoscopic examination revealed:
• Diffuse erythema
• Fine scaling
• Superficial epidermal disruption
• No features suggestive of psoriasis
Diagnosis
Based on clinical findings, exposure history, dermatological examination, and patch test results, a diagnosis of: Allergic Contact Dermatitis Secondary to Household Cleaning Agents was established.
Management and Outcome
Initial Management
The patient was advised:
• Immediate avoidance of triggering cleaning agents
• Use of protective gloves during household work
• Regular application of emollients
• Skin barrier protection measures
Medical Therapy
Treatment included:
• Topical Mometasone Furoate 0.1% cream once daily
• Intensive moisturization with ceramide-containing emollients
• Oral Cetirizine 10 mg daily for itching
• Soap substitutes for hand hygiene
The patient was educated regarding avoidance of fragranced products and potential cross-reactive allergens.
Hospital Course
At 1 Week
• Significant reduction in itching
• Decreased erythema
• Improved skin hydration
At 3 Weeks
• Marked reduction in scaling
• Healing of fissures
• Resolution of burning sensation
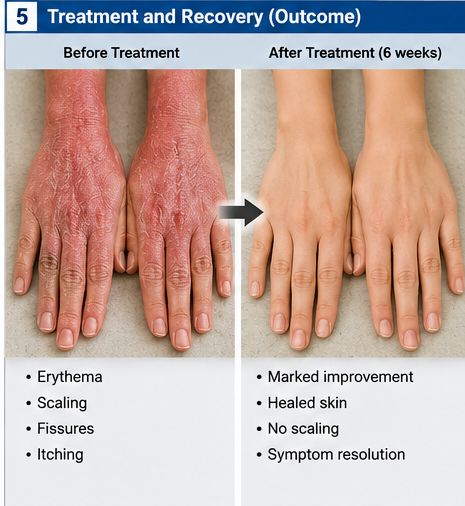
At 6 Weeks
• Near-complete resolution of lesions
• No new eruptions
• Restoration of normal skin texture
Follow-Up
At 3 Months
• Complete symptom resolution
• No recurrence
• Excellent compliance with allergen avoidance measures
• Improved quality of life
Discussion
Pathophysiology
Contact dermatitis develops when environmental agents disrupt skin barrier integrity or induce an immune-mediated inflammatory response.
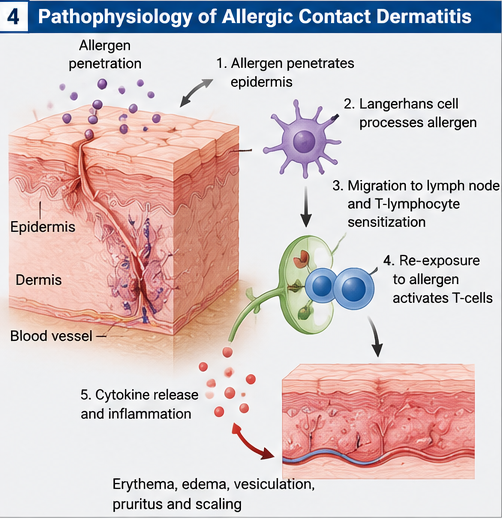
In allergic contact dermatitis:
• Allergens penetrate the epidermis
• Langerhans cells process allergens
• Sensitization of T lymphocytes occurs
• Re-exposure triggers delayed hypersensitivity
• Inflammatory cytokines produce dermatitis
The resulting inflammatory response causes erythema, itching, edema, and epidermal damage.
Epidemiology
Important epidemiological features include:
• One of the most common occupational skin disorders
• More frequent among women
• Common in healthcare workers
• Common in cleaning professionals
• Significant impact on quality of life
• Increasing prevalence due to exposure to chemicals and cosmetic products
Clinical Manifestations
Common symptoms include:
• Pruritus
• Erythema
• Scaling
• Burning sensation
• Edema
• Vesiculation
• Fissuring
• Dry skin
Chronic disease may result in:
• Lichenification
• Hyperpigmentation
• Secondary infection
• Persistent eczema
Diagnostic Considerations
Diagnosis relies on:
- Detailed exposure history
- Clinical examination
- Identification of triggers
- Patch testing
- Exclusion of fungal infections
- Dermatological assessment
Patch testing remains the gold standard for confirming allergic contact dermatitis.
Treatment Modalities
Medical Therapy
Most patients respond to:
• Topical corticosteroids
• Emollients
• Antihistamines
• Barrier repair therapies
Allergen Avoidance
The most important intervention includes:
• Identification of offending allergens
• Avoidance of exposure
• Use of protective equipment
• Patient education
Systemic Therapy
Reserved for:
• Severe disease
• Extensive dermatitis
• Refractory cases
Potential options include:
• Oral corticosteroids
• Immunosuppressive therapy
• Biologic agents in selected cases
Complications
Potential complications include:
• Chronic eczema
• Secondary bacterial infection
• Skin fissuring
• Occupational disability
• Sleep disturbance
• Reduced quality of life
Early diagnosis significantly reduces long-term morbidity.
Prognosis
Prognosis depends upon:
• Early identification of allergens
• Patient compliance
• Severity of exposure
• Chronicity of disease
• Adequacy of skin protection
Most patients achieve excellent outcomes when trigger avoidance and appropriate therapy are implemented.
Conclusion
Contact dermatitis remains a common but often preventable inflammatory skin disorder. Careful exposure history, thorough clinical evaluation, and patch testing are critical for accurate diagnosis and identification of causative allergens. This case demonstrates the successful management of allergic contact dermatitis through allergen avoidance, topical corticosteroid therapy, skin barrier restoration, and patient education. Early recognition and preventive measures remain essential for preventing chronic disease, minimizing complications, and ensuring favorable long-term outcomes.
References
- Fonacier L, Bernstein DI, Pacheco K, et al. Contact Dermatitis: A Practice Parameter Update 2015. J Allergy Clin Immunol Pract. 2015;3(3):S1-S39. https://www.jaci-inpractice.org/article/S2213-2198(15)00195-3/fulltext
- Johansen JD, Aalto-Korte K, Agner T, et al. European Society of Contact Dermatitis guideline for diagnostic patch testing. Contact Dermatitis. 2015;73(4):195-221. https://pubmed.ncbi.nlm.nih.gov/26395552/
- Thyssen JP, Linneberg A, Menné T, Johansen JD. The epidemiology of contact allergy in the general population. Contact Dermatitis. 2007;57(5):287-299. https://pubmed.ncbi.nlm.nih.gov/17937743/
- Usatine RP, Riojas M. Diagnosis and Management of Contact Dermatitis. Am Fam Physician. 2010;82(3):249-255. https://www.aafp.org/pubs/afp/issues/2010/0801/p249.html
- Belsito DV. Occupational Contact Dermatitis: Etiology, Prevalence, and Resulting Impairment. Am J Contact Dermat. 2005;16(3):111-116. https://pubmed.ncbi.nlm.nih.gov/16191004/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge