Organ Transplantation: Opportunistic Infection Following Renal Transplantation – A Case Report
OthersPage Navigation
Abstract
Organ transplantation has revolutionized the management of end-stage organ failure, significantly improving survival and quality of life. However, long-term immunosuppressive therapy, which is essential to prevent graft rejection, predisposes transplant recipients to various opportunistic infections. These infections remain a major cause of morbidity and mortality following transplantation and often present with atypical clinical manifestations.
We present the case of a 48-year-old male renal transplant recipient who developed pulmonary cytomegalovirus (CMV) infection six months after transplantation while receiving maintenance immunosuppressive therapy. The patient presented with fever, progressive breathlessness, nonproductive cough, and generalized weakness. Clinical evaluation, laboratory investigations, radiological imaging, and polymerase chain reaction (PCR) testing confirmed CMV pneumonitis. Prompt initiation of antiviral therapy resulted in significant clinical improvement and preservation of graft function.
This case highlights the importance of early recognition, vigilant surveillance, and timely management of opportunistic infections in organ transplant recipients.
Introduction
Organ transplantation is the definitive treatment for many patients with end-stage renal, hepatic, cardiac, and pulmonary diseases. Advances in surgical techniques, donor matching, and immunosuppressive medications have significantly improved graft survival and patient outcomes.
Despite these advancements, immunosuppressive therapy creates a state of impaired cellular and humoral immunity, increasing susceptibility to opportunistic infections. These infections are caused by microorganisms that rarely cause disease in immunocompetent individuals but can become life-threatening in transplant recipients.
Common opportunistic infections following transplantation include:
• Cytomegalovirus (CMV)
• Pneumocystis jirovecii pneumonia (PJP)
• Aspergillosis
• Candidiasis
• BK virus nephropathy
• Tuberculosis
• Nocardiosis
• Herpes simplex virus infection
• Varicella-zoster virus infection
The risk of infection is highest during the first year after transplantation, particularly within the first six months when immunosuppression is most intense.
Early diagnosis is often challenging because symptoms may be nonspecific and overlap with graft rejection or medication-related adverse effects.
Case Report
Patient History
A 48-year-old male presented to the transplant medicine clinic with complaints of:
• Persistent fever for 10 days
• Progressive shortness of breath
• Dry cough
• Generalized fatigue
• Reduced appetite
The patient had undergone living-donor renal transplantation six months earlier for end-stage kidney disease secondary to diabetic nephropathy.
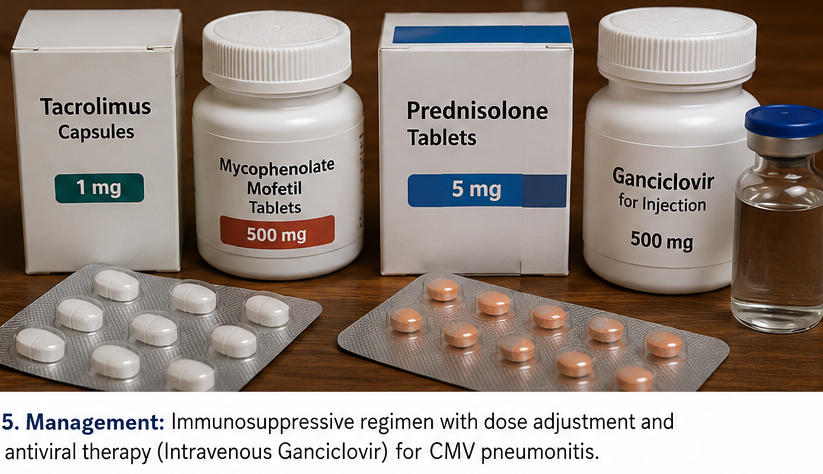
Current medications included:
• Tacrolimus
• Mycophenolate mofetil
• Prednisolone
The patient had completed routine postoperative follow-up and initially demonstrated excellent graft function.
There was no recent travel history or known exposure to tuberculosis.
Clinical Examination
General Examination
• Blood pressure: 128/78 mmHg
• Pulse rate: 96/min
• Respiratory rate: 22/min
• Temperature: 101.4°F
• Oxygen saturation: 93% on room air
The patient appeared fatigued and mildly dyspneic.
Respiratory Examination
Findings included:
• Bilateral fine inspiratory crackles
• Reduced air entry at lung bases
• No wheezing
• Mild tachypnea
Cardiovascular and abdominal examinations were unremarkable.
The transplanted kidney was non-tender and functioning adequately.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Cytomegalovirus pneumonitis
• Pneumocystis jirovecii pneumonia
• Bacterial pneumonia
• Pulmonary tuberculosis
• Fungal pneumonia
• Acute graft rejection with pulmonary manifestations
Given the patient's immunosuppressed status and timing after transplantation, opportunistic infection was strongly suspected.
Investigations
Laboratory Evaluation
Results showed:
• Hemoglobin: 11.4 g/dL
• Total leukocyte count: 3,200/mm³
• Platelet count: 156,000/mm³
• Serum creatinine: 1.3 mg/dL
• C-reactive protein: 42 mg/L
• ESR: 38 mm/hr
• Elevated liver enzymes
The presence of leukopenia raised suspicion for viral infection.
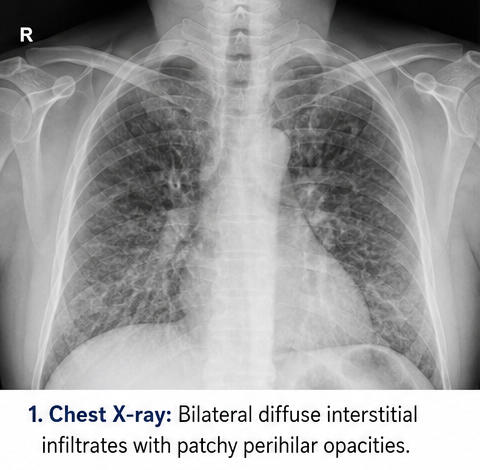
Chest Radiography
Chest X-ray demonstrated:
• Bilateral diffuse interstitial infiltrates
• Patchy perihilar opacities
High-Resolution CT Scan
HRCT revealed:
• Bilateral ground-glass opacities
• Patchy interstitial infiltrates
• No cavitary lesions
• No pleural effusion

Microbiological Evaluation
The following tests were performed:
• Blood cultures – Negative
• Sputum bacterial cultures – Negative
• Tuberculosis testing – Negative
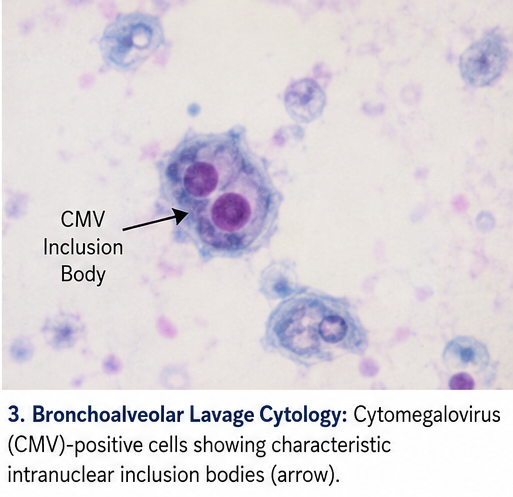
• Fungal cultures – NegativeBronchoalveolar Lavage
Bronchoscopy with lavage showed:
• CMV-positive cells
• Absence of Pneumocystis jirovecii
• No fungal organisms
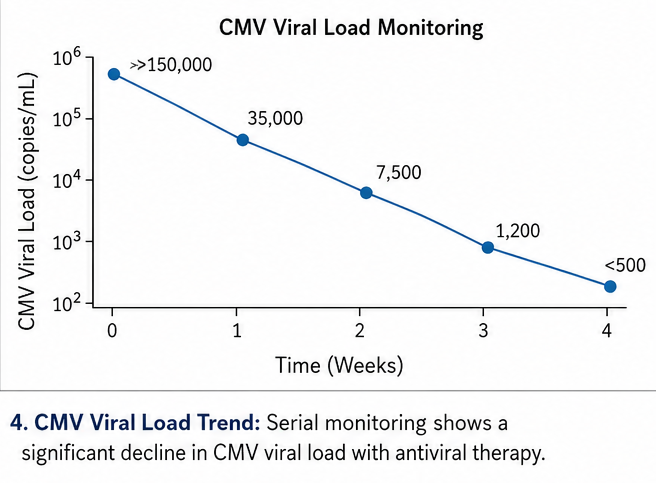
CMV Testing
Quantitative CMV PCR demonstrated:
• CMV viral load >150,000 copies/mL
CMV antigenemia testing was positive.
Diagnosis
Based on clinical findings, imaging studies, and virological confirmation, a diagnosis of: Cytomegalovirus Pneumonitis Following Renal Transplantation was established.
Management and Outcome
Initial Management
The patient was admitted to the transplant unit.
Treatment included:
• Intravenous ganciclovir
• Temporary reduction of mycophenolate dosage
• Continuation of tacrolimus with close monitoring
• Supplemental oxygen therapy
• Intravenous hydration
Close monitoring of graft function and blood counts was performed throughout hospitalization.
Hospital Course
At 1 Week
• Fever subsided
• Improvement in oxygen saturation
• Reduced respiratory symptoms
• Decreasing viral load
At 2 Weeks
• Significant improvement in exercise tolerance
• Resolution of cough
• Normalization of inflammatory markers
At 3 Weeks
• CMV viral load markedly reduced
• Stable graft function
• Improved appetite and energy levels
Follow-Up
At 3 Months
• Complete resolution of pulmonary symptoms
• Undetectable CMV viral load
• Stable renal function
• No evidence of graft rejection
The patient remained compliant with antiviral prophylaxis and follow-up surveillance.
Discussion
Immunosuppression and Opportunistic Infections
Successful transplantation depends on long-term immunosuppression. However, suppression of T-cell-mediated immunity predisposes recipients to infections that are uncommon in healthy individuals.
The risk of opportunistic infection depends on:
• Degree of immunosuppression
• Time since transplantation
• Donor-recipient viral status
• Presence of comorbidities
• Environmental exposure
Among these infections, CMV remains one of the most clinically significant pathogens affecting transplant recipients.
Cytomegalovirus Infection
CMV is a double-stranded DNA virus belonging to the herpesvirus family.
In transplant recipients, CMV may cause:
• Pneumonitis
• Colitis
• Hepatitis
• Retinitis
• Bone marrow suppression
• Graft dysfunction
CMV infection also increases susceptibility to secondary bacterial and fungal infections.
Other Common Opportunistic Infections
Pneumocystis jirovecii Pneumonia (PJP)
Characterized by:
• Progressive dyspnea
• Dry cough
• Hypoxemia
• Ground-glass opacities on imaging
Aspergillosis
Often presents with:
• Fever
• Hemoptysis
• Pulmonary nodules
• Invasive disease
BK Virus Infection
May result in:
• Polyomavirus nephropathy
• Progressive graft dysfunction
Tuberculosis
Particularly common in developing countries and may present atypically in transplant recipients.
Diagnostic Considerations
Early diagnosis requires:
- High clinical suspicion
- Regular surveillance testing
- Molecular diagnostic techniques
- Imaging studies
- Microbiological confirmation
PCR-based viral testing has significantly improved the detection of CMV disease.
Prevention Strategies
Important preventive measures include:
• Antiviral prophylaxis
• Regular CMV monitoring
• Appropriate immunosuppressive dosing
• Infection surveillance
• Vaccination when indicated
• Patient education regarding infection prevention
Complications
Untreated opportunistic infections may result in:
• Respiratory failure
• Sepsis
• Multi-organ dysfunction
• Graft rejection
• Graft loss
• Death
Prompt diagnosis and treatment substantially improve outcomes.
Prognosis
The prognosis depends upon:
• Early recognition
• Timely antiviral therapy
• Severity of infection
• Preservation of graft function
• Patient adherence to follow-up
With modern diagnostic tools and antiviral treatment, most patients can achieve favorable long-term outcomes while maintaining graft survival.
Conclusion
Organ transplantation remains a life-saving intervention for patients with end-stage organ failure; however, opportunistic infections continue to pose significant challenges during the post-transplant period. This case demonstrates the importance of maintaining a high index of suspicion for CMV infection in transplant recipients presenting with respiratory symptoms and systemic illness. Early diagnosis through molecular testing, appropriate antiviral therapy, and careful adjustment of immunosuppressive medications resulted in successful recovery and preservation of graft function. Continuous surveillance, preventive strategies, and multidisciplinary management remain essential for reducing infection-related morbidity and mortality in transplant recipients.
References
- Fishman JA. Infection in Organ Transplantation. Am J Transplant. 2017;17(4):856-879. https://pubmed.ncbi.nlm.nih.gov/27873480/
- Kotton CN. CMV: Prevention, Diagnosis and Therapy. Am J Transplant. 2013;13(Suppl 3):24-40. https://pubmed.ncbi.nlm.nih.gov/23465003/
- Razonable RR, Humar A. Cytomegalovirus in Solid Organ Transplantation. Am J Transplant. 2013;13(Suppl 4):93-106. https://pubmed.ncbi.nlm.nih.gov/23465011/
- Fishman JA, Gans H. Pneumocystis jirovecii in Solid Organ Transplantation. Am J Transplant. 2019;19(2):311-320. https://pubmed.ncbi.nlm.nih.gov/30281895/
- Avery RK. Infections After Organ Transplantation. Clin Chest Med. 2017;38(4):717-728. https://pubmed.ncbi.nlm.nih.gov/29128039/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge