Viral Exanthema in Children: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Viral exanthema is a common pediatric condition characterized by widespread skin eruptions associated with systemic viral infections. These exanthematous illnesses frequently affect infants and children and are commonly caused by viruses such as measles, rubella, parvovirus B19, enteroviruses, adenovirus, human herpesvirus-6 (HHV-6), and Epstein–Barr virus. Clinical manifestations typically include fever, diffuse erythematous rash, malaise, upper respiratory symptoms, irritability, and lymphadenopathy. Although most cases are self-limiting, early recognition is essential to differentiate viral exanthema from bacterial infections, allergic drug eruptions, autoimmune conditions, and other serious pediatric illnesses.
We present the case of a 6-year-old male child who presented with fever, generalized erythematous rash, pruritus, and upper respiratory symptoms for four days. Clinical examination and laboratory evaluation supported the diagnosis of viral exanthema, most likely secondary to enteroviral infection. The child was managed conservatively with symptomatic treatment, hydration, antipyretics, antihistamines, and parental counseling, resulting in complete clinical recovery without complications.
This case highlights the importance of accurate clinical assessment, exclusion of severe infectious etiologies, supportive care, and patient monitoring in the management of pediatric viral exanthema.
Introduction
Viral exanthema refers to a diffuse skin eruption caused by systemic viral infections. It is among the most common dermatological presentations in pediatric practice and often accompanies febrile illnesses in children. Viral exanthems are usually benign and self-limiting; however, their clinical presentation may overlap with life-threatening infectious diseases, making early diagnosis clinically important.
Common viruses associated with pediatric viral exanthema include:
- Measles virus
- Rubella virus
- Human herpesvirus-6 (Roseola infantum)
- Enteroviruses
- Parvovirus B19
- Adenovirus
- Epstein–Barr virus
- Varicella-zoster virus
The rash pattern may vary depending on the underlying viral pathogen and immune response. Exanthems may present as maculopapular, vesicular, morbilliform, petechial, or urticarial eruptions.
Predisposing and associated factors include:
- Exposure to infected individuals
- Poor immunity
- Crowded environments
- Lack of vaccination
- Seasonal viral outbreaks
- School exposure
- Malnutrition
Common clinical manifestations include:
- Fever
- Generalized rash
- Coryza
- Cough
- Sore throat
- Pruritus
- Irritability
- Fatigue
- Reduced appetite
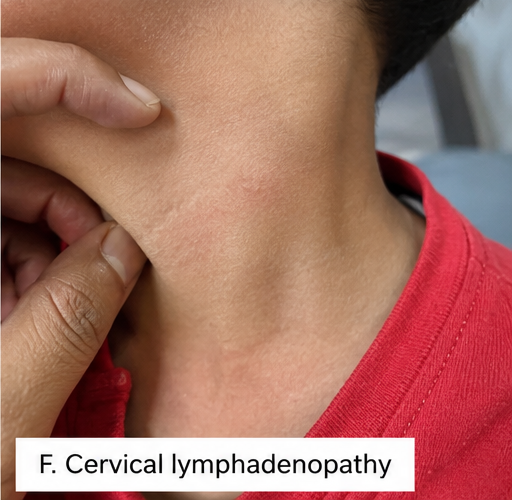
- Cervical lymphadenopathy
Most viral exanthems resolve spontaneously with supportive management. However, prompt identification remains essential to avoid complications and unnecessary antibiotic use.
Case Report
Patient History
A 6-year-old male child was brought to the pediatric outpatient department with:
- Fever for four days
- Generalized reddish skin rash
- Mild itching over the trunk and extremities
- Runny nose and sore throat
- Decreased appetite
- Fatigue and irritability
The rash initially appeared over the face and upper chest before spreading to the trunk, back, and limbs over 24 hours.
There was no history of:
- Breathing difficulty
- Seizures
- Drug intake prior to rash onset
- Recent vaccination
- Joint pain
- Bleeding manifestations
Past medical history was unremarkable, and immunization status was appropriate for age.
Clinical Examination
General Examination
Clinical examination revealed:
- Conscious and active child
- Mild fever
- Pulse rate: 102/min
- Respiratory rate: 22/min
- Mild dehydration
- No respiratory distress
Dermatological Examination
Cutaneous examination demonstrated:
- Diffuse erythematous maculopapular rash
- Rash involving face, trunk, back, and extremities
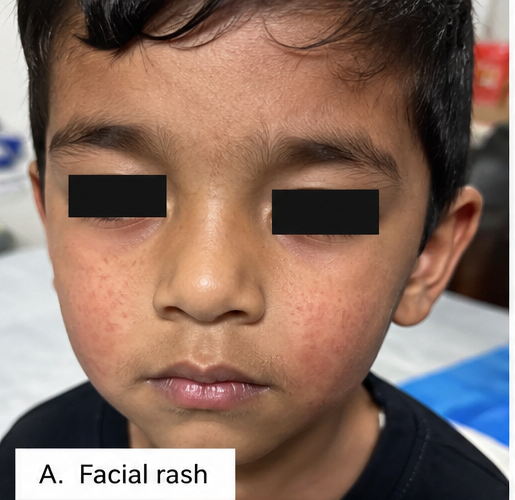

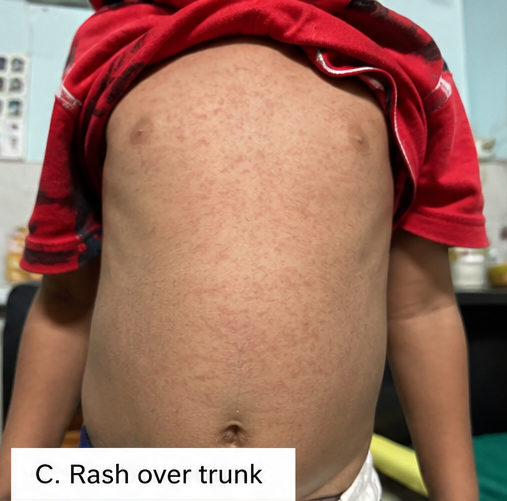
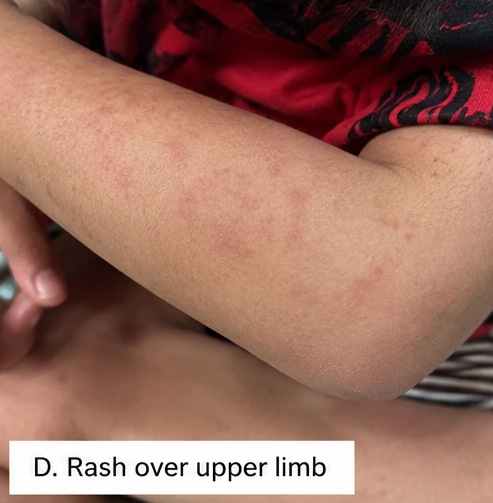

- Blanching lesions
- Mild pruritus
- No vesicles or pustules
- No mucosal ulceration
- No skin peeling
Mild cervical lymphadenopathy was present.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
- Viral exanthema
- Measles
- Rubella
- Scarlet fever
- Drug-induced rash
- Kawasaki disease
- Dengue fever
- Allergic dermatitis
The diffuse blanching maculopapular rash associated with upper respiratory symptoms strongly favored viral exanthema.
Investigations
Laboratory Findings
Initial laboratory investigations revealed:
- Mild leukopenia
- Normal platelet count
- Mildly elevated C-reactive protein
- Normal liver and renal function tests
Viral Evaluation
Additional evaluation demonstrated:
- Negative dengue serology
- Negative rapid streptococcal antigen test
- No evidence of bacterial infection
Based on clinical findings and laboratory correlation, enteroviral viral exanthema was considered the most likely diagnosis.
Diagnosis
Based on clinical presentation, characteristic rash pattern, systemic viral symptoms, and exclusion of bacterial and other infectious causes, a diagnosis of Pediatric Viral Exanthema was established.
Management and Outcome
Initial Medical Management
The child was managed conservatively with:
- Oral paracetamol for fever
- Oral antihistamines for itching
- Adequate oral hydration
- Nutritional support
- Skin care measures
- Rest and observation
Parents were counseled regarding:
- Fever monitoring
- Hydration maintenance
- Avoidance of unnecessary antibiotics
- Proper hygiene practices
- Warning signs requiring urgent medical attention
No antiviral therapy was required.
Follow-Up and Clinical Course
At 5 Days
- Significant reduction in fever
- Rash fading gradually
- Improved appetite
- Reduced irritability
At 10 Days
- Near-complete resolution of rash
- No new lesions
- Normal activity level restored
- No secondary infection observed
At 3 Weeks
- Complete recovery achieved
- No pigmentation or scarring
- No recurrence of symptoms
The child remained clinically stable during follow-up.
Discussion
Pathophysiology
Viral exanthema develops due to systemic viral infection and immune-mediated inflammatory responses within the skin. Viral replication triggers cytokine release, vascular dilation, and inflammatory cell infiltration, resulting in diffuse cutaneous eruptions.
Important pathological mechanisms include:
- Viral dissemination through bloodstream
- Immune activation
- Cytokine-mediated inflammation
- Dermal vascular response
- Epidermal immune reaction
The morphology and distribution of rash vary according to the infecting virus and host immune response.
Epidemiology
Important epidemiological features include:
- Common in pediatric age groups
- Frequently associated with seasonal outbreaks
- Higher incidence in school-going children
- Viral respiratory infections are common triggers
- Most cases are self-limiting
Viral exanthems contribute substantially to pediatric outpatient visits worldwide.
Clinical Manifestations
Clinical presentation varies according to viral etiology.
Common manifestations include:
- Fever
- Maculopapular rash
- Coryza
- Sore throat
- Malaise
- Fatigue
- Pruritus
- Lymphadenopathy
- Reduced appetite
Certain viral infections may additionally present with conjunctivitis, oral lesions, or gastrointestinal symptoms.
Diagnostic Considerations
Important diagnostic modalities include:
- Detailed clinical examination
- Rash morphology assessment
- Viral exposure history
- Laboratory evaluation
- Serological testing when indicated
- Exclusion of bacterial infections
Most uncomplicated viral exanthems are diagnosed clinically without extensive investigations.
Treatment Modalities
Supportive Management
Supportive care remains the cornerstone of treatment and includes:
- Hydration
- Antipyretics
- Antihistamines
- Nutritional support
- Skin care
- Rest
Pharmacological Therapy
Commonly used medications include:
- Paracetamol
- Cetirizine
- Calamine lotion
- Oral fluids and electrolyte solutions
Antibiotics are generally not indicated unless secondary bacterial infection develops.
Preventive Measures
Preventive strategies include:
- Vaccination
- Hand hygiene
- Isolation during active infection
- Avoiding school attendance during fever
- Respiratory hygiene practices
- Proper nutrition
Early recognition helps reduce transmission and complications.
Complications
Although most cases are benign, potential complications include:
- Dehydration
- Secondary bacterial skin infection
- Febrile seizures
- Pneumonia
- Encephalitis (rare)
- Persistent fever
Complications are more common in immunocompromised children.
Prognosis
The prognosis of uncomplicated viral exanthema in children is generally excellent.
Important prognostic factors include:
- Early diagnosis
- Adequate hydration
- Supportive management
- Nutritional status
- Immune competence
- Timely monitoring for complications
Most children recover completely without long-term sequelae.
Conclusion
Viral exanthema is a common pediatric viral illness characterized by diffuse rash and systemic symptoms that can mimic several infectious and inflammatory conditions. Accurate clinical assessment, exclusion of serious illnesses, supportive management, hydration, and parental counseling remain essential for successful treatment. This case highlights the importance of recognizing characteristic rash patterns and avoiding unnecessary antibiotic use in uncomplicated pediatric viral exanthema.
References
- World Health Organization. Measles and viral exanthematous illnesses. https://www.who.int/
- Centers for Disease Control and Prevention. Viral Rash Illnesses in Children. https://www.cdc.gov/
- Cherry JD, Harrison GJ. Feigin and Cherry’s Textbook of Pediatric Infectious Diseases. https://pubmed.ncbi.nlm.nih.gov/
- Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. https://pubmed.ncbi.nlm.nih.gov/
- American Academy of Pediatrics. Viral Exanthems in Childhood. https://publications.aap.org/
- DermNet NZ. Viral Skin Infections and Exanthems. https://dermnetnz.org/
- Leung AKC, Barankin B, Hon KLE. Viral exanthems in childhood: an update. https://pubmed.ncbi.nlm.nih.gov/30273242/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge