Frictional Hyperkeratosis: Localized Plantar Skin Thickening Secondary to Chronic Mechanical Stress – A Case Report
OthersPage Navigation
Abstract
Frictional hyperkeratosis is a benign acquired dermatological condition characterized by localized thickening of the stratum corneum in response to repeated friction, pressure, or mechanical trauma. It commonly affects the palms, soles, knuckles, and other areas subjected to chronic irritation. Although often considered a minor dermatological problem, frictional hyperkeratosis may cause significant pain, discomfort, impaired mobility, and reduced quality of life. Early diagnosis and correction of underlying mechanical factors are essential for successful treatment and prevention of recurrence.
We present the case of a 42-year-old male factory worker who developed progressive thickening and pain over the plantar aspect of the right forefoot. Clinical examination revealed a well-demarcated hyperkeratotic plaque associated with tenderness during weight-bearing activities. Dermoscopic examination supported the diagnosis of frictional hyperkeratosis and helped exclude plantar wart and other differential diagnoses. Conservative treatment consisting of keratolytic therapy, mechanical debridement, footwear modification, pressure offloading, and patient education resulted in significant improvement and complete symptom resolution.
This case highlights the importance of recognizing chronic mechanical stress as an underlying cause of frictional hyperkeratosis and demonstrates the effectiveness of conservative management in achieving favorable long-term outcomes.
Introduction
Frictional hyperkeratosis is a reactive thickening of the epidermis that develops in response to chronic mechanical friction or repetitive pressure. The condition represents a physiological protective mechanism whereby the skin increases keratin production to protect deeper tissues from repeated trauma. While this adaptive response initially serves a protective role, excessive keratin accumulation can eventually lead to discomfort, pain, cosmetic concerns, and functional limitations.
The condition is particularly common among individuals whose occupations or daily activities involve prolonged standing, repetitive manual labor, sports participation, or the use of poorly fitting footwear. Areas most frequently affected include the plantar surfaces of the feet, palms, fingers, knuckles, elbows, and pressure-bearing bony prominences.
Several risk factors contribute to the development of frictional hyperkeratosis, including:
• Ill-fitting footwear
• Repetitive occupational activities
• Prolonged standing
• Obesity
• Abnormal gait patterns
• Foot deformities
• Sports-related repetitive trauma
• Improper weight distribution during walking
Patients typically present with localized thickened skin that may be asymptomatic initially but can become painful with continued pressure. Differentiating frictional hyperkeratosis from corns, calluses, plantar warts, psoriasis, and inherited keratodermas is important to ensure appropriate management.
Case Report
Patient History
A 42-year-old male factory worker presented to the dermatology outpatient department with complaints of:
• Thickened skin over the ball of the right foot
• Pain while walking for four months
• Discomfort during prolonged standing
• Difficulty wearing certain types of footwear
• Progressive increase in lesion thickness
The patient reported that symptoms began gradually and had worsened over time. He worked in a manufacturing unit where he remained standing for approximately 10–12 hours daily. He denied any acute trauma or injury to the foot.
The patient had attempted self-treatment using over-the-counter moisturizers without significant improvement.

Past medical history was unremarkable.
There was no history of:
• Diabetes mellitus
• Peripheral vascular disease
• Psoriasis
• Rheumatological disorders
• Previous foot surgery
• Similar lesions elsewhere
Family history was non-contributory.
Clinical Examination
General physical examination was normal.
Vital signs were stable:
• Blood pressure: 128/82 mmHg
• Pulse rate: 76 beats/minute
• Temperature: Afebrile
Local examination revealed:
• A well-circumscribed hyperkeratotic plaque measuring approximately 2.5 × 2 cm
• Yellowish discoloration of thickened skin
• Mild tenderness on direct pressure
• Preserved surrounding skin architecture
• No erythema or discharge
• No ulceration or bleeding
The lesion was firm, non-mobile, and localized to the plantar forefoot region.
Gait analysis demonstrated increased pressure loading over the metatarsal heads during ambulation.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Frictional hyperkeratosis
• Plantar callus
• Corn (clavus)
• Plantar wart (verruca plantaris)
• Palmoplantar keratoderma
• Psoriasis
• Foreign body granuloma
The characteristic location, occupational history, and clinical appearance strongly favored frictional hyperkeratosis.
Investigations
Laboratory Evaluation
Routine laboratory investigations revealed:
• Hemoglobin: 14.1 g/dL
• White blood cell count: 7,100/mm³
• ESR: 12 mm/hr
• Fasting blood glucose: 94 mg/dL
• HbA1c: 5.4%
All values were within normal limits.
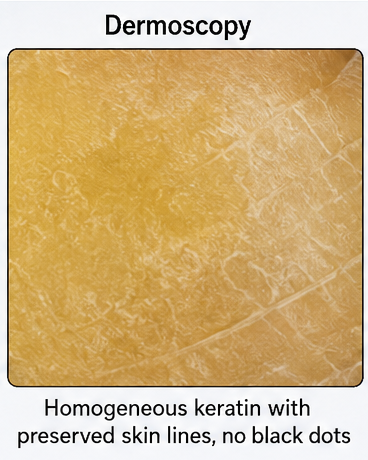
Dermoscopic Examination
Dermoscopy demonstrated:
• Homogeneous yellow keratin accumulation
• Preserved skin lines
• Absence of thrombosed capillaries
• No punctate hemorrhages
These findings helped differentiate the lesion from plantar warts.
Radiographic Evaluation
Plain radiographs of the foot showed:
• Normal bony architecture
• No fracture or deformity
• No retained foreign body
• Preserved joint spaces
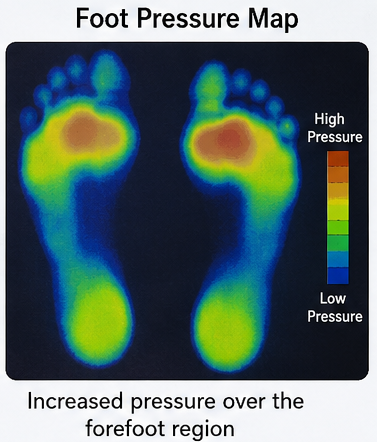
Foot Pressure Map
Foot pressure mapping demonstrated increased plantar pressure over the forefoot region, corresponding to the site of hyperkeratosis. The abnormal pressure distribution supported chronic mechanical stress as the underlying cause of the lesion and guided the use of pressure-relieving insoles as part of the treatment plan.
Diagnosis
Based on clinical, dermoscopic, and radiological findings, the patient was diagnosed with: Frictional Hyperkeratosis of the Plantar Forefoot Secondary to Chronic Mechanical Pressure
Management and Outcome
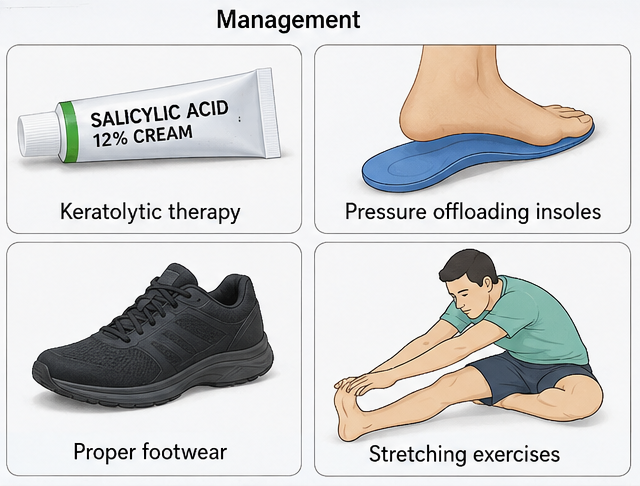
Initial Treatment
The patient was managed conservatively with:
• Topical salicylic acid 12% cream
• Urea-based moisturizer
• Mechanical debridement of excess keratin
• Pressure-relieving insoles
• Footwear modification
• Activity modification
• Patient education regarding foot care
The patient was advised to use cushioned footwear and avoid prolonged standing whenever possible.
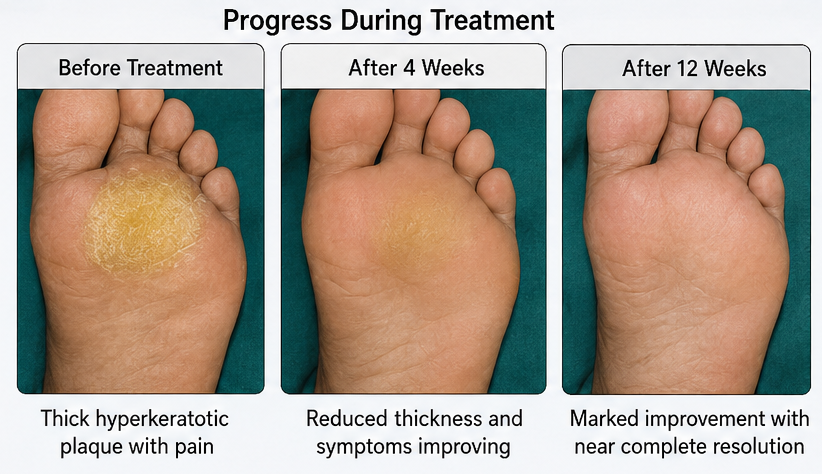
Clinical Course
After four weeks of treatment:
• Pain significantly decreased
• Walking became more comfortable
• Lesion thickness reduced noticeably
• Tenderness improved substantially
No adverse effects were observed.
Follow-Up
At 4 Weeks
The patient reported:
• Approximately 60% reduction in symptoms
• Improved mobility
• Reduced discomfort during work
At 12 Weeks
Clinical examination demonstrated:
• Marked reduction in hyperkeratosis
• Near-complete symptom resolution
• Restoration of normal daily activities
At 18 Weeks
Long-term follow-up revealed:
• No recurrence
• Continued use of pressure-relieving footwear
• Sustained clinical improvement
Discussion
Frictional hyperkeratosis develops as a protective response to repeated mechanical stress. Chronic friction stimulates increased proliferation of keratinocytes, resulting in excessive accumulation of keratin within the stratum corneum. Over time, this adaptive response produces visible thickening of the skin and may become symptomatic.
The plantar foot is particularly susceptible because it is continuously exposed to body weight and repetitive pressure during walking and standing. Occupations involving prolonged standing, such as factory work, retail work, healthcare services, and construction labor, increase the risk of developing friction-induced skin lesions.
Clinical diagnosis is usually straightforward; however, differentiation from plantar warts is essential. Plantar warts typically interrupt normal skin lines and contain thrombosed capillaries visible on dermoscopy. In contrast, frictional hyperkeratosis preserves normal dermatoglyphics and lacks vascular structures.
Clinical Features
Common manifestations include:
• Localized skin thickening
• Yellow or gray hyperkeratotic plaques
• Pain during walking
• Pressure-induced tenderness
• Cosmetic concerns
• Difficulty wearing footwear
Differential Diagnosis
Plantar Wart: Characterized by thrombosed capillaries and disruption of skin lines.
Corn (Clavus): Usually presents with a central keratin core causing focal pain.
Palmoplantar Keratoderma: Often hereditary and diffuse rather than localized.
Psoriasis: Associated with erythematous scaly plaques and involvement of multiple body sites.
Treatment
Management focuses on eliminating the source of friction and reducing excessive keratin accumulation.
Common therapeutic measures include:
• Keratolytic agents (salicylic acid, urea)
• Mechanical debridement
• Proper footwear
• Orthotic support
• Pressure redistribution devices
• Weight reduction when appropriate
• Patient education
Most patients respond well to conservative treatment. Surgical intervention is rarely required.
Complications
Untreated frictional hyperkeratosis may lead to:
• Chronic pain
• Recurrent lesions
• Skin fissuring
• Secondary infection
• Functional limitation
• Reduced quality of life
Early intervention significantly reduces these risks.
Prognosis
The prognosis of frictional hyperkeratosis is excellent when the underlying mechanical cause is identified and corrected. Most patients experience substantial symptom improvement within weeks of treatment. Long-term prevention depends on maintaining appropriate footwear, pressure redistribution, and regular skin care. Recurrence is common if frictional forces persist.
Conclusion
Frictional hyperkeratosis is a common benign skin disorder resulting from chronic friction and repetitive mechanical stress. Although often overlooked, it can significantly affect comfort, mobility, and quality of life. This case demonstrates the importance of clinical recognition, dermoscopic evaluation, and identification of occupational risk factors. Conservative management consisting of keratolytic therapy, pressure offloading, footwear modification, and patient education can achieve excellent clinical outcomes while preventing recurrence.
References
- Sterling JC, Handfield-Jones S, Hudson PM. Guidelines for the management of cutaneous warts. Br J Dermatol. 2001;144(1):4-11. https://pubmed.ncbi.nlm.nih.gov/11167676/
- Yosipovitch G, Fleischer AB Jr. Hyperkeratotic disorders of the feet. Clin Dermatol. 2001;19(3):285-289. https://pubmed.ncbi.nlm.nih.gov/11388672/
- American Academy of Dermatology. Corns and Calluses: Diagnosis and Treatment. https://www.aad.org/public/diseases/a-z/corns-and-calluses-treatment
- Rook's Textbook of Dermatology. 9th Edition. Wiley-Blackwell; 2016.
- MedlinePlus. Hyperkeratosis Overview. https://medlineplus.gov
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge