Pulmonary Aspergillosis in an Immunocompromised Patient Presenting with Persistent Cough and Hemoptysis: A Case Report
OthersPage Navigation
Abstract
Pulmonary aspergillosis is a fungal infection caused primarily by Aspergillus fumigatus, a ubiquitous environmental mold that can produce a wide spectrum of respiratory diseases depending on host immune status and underlying lung pathology. Clinical manifestations range from allergic bronchopulmonary aspergillosis and chronic pulmonary aspergillosis to life-threatening invasive aspergillosis. Early diagnosis remains challenging because symptoms are often nonspecific and may mimic bacterial pneumonia, tuberculosis, or malignancy.
We report the case of a 58-year-old male with poorly controlled diabetes mellitus who presented with persistent cough, low-grade fever, weight loss, and intermittent hemoptysis. Computed tomography of the chest demonstrated a cavitary lesion in the right upper lobe containing a mobile intracavitary mass suggestive of aspergilloma. Microbiological and serological investigations supported the diagnosis of chronic pulmonary aspergillosis. The patient was treated with oral voriconazole and showed significant clinical and radiological improvement during follow-up.
This case highlights the importance of considering pulmonary aspergillosis in patients with chronic respiratory symptoms and predisposing risk factors. Timely diagnosis and appropriate antifungal therapy are essential for favorable outcomes.
Introduction
Aspergillosis refers to a group of diseases caused by fungi belonging to the genus Aspergillus. Among the more than 300 identified species, Aspergillus fumigatus is responsible for most human infections. These organisms are commonly found in soil, decaying vegetation, dust, and indoor environments. Humans are routinely exposed to airborne fungal spores; however, disease usually develops only when host defense mechanisms are impaired or when structural lung abnormalities are present.
Pulmonary aspergillosis is one of the most common manifestations of aspergillus infection. The disease spectrum includes:
• Allergic bronchopulmonary aspergillosis (ABPA)
• Chronic pulmonary aspergillosis (CPA)
• Aspergilloma (fungal ball)
• Invasive pulmonary aspergillosis (IPA)
• Aspergillus bronchitis
Risk factors include:
• Diabetes mellitus
• Chronic obstructive pulmonary disease
• Previous pulmonary tuberculosis
• Long-term corticosteroid therapy
• Hematological malignancies
• Organ transplantation
• Neutropenia
Patients may present with chronic cough, sputum production, chest pain, fatigue, dyspnea, fever, and hemoptysis. Because the clinical features overlap with many pulmonary diseases, a combination of imaging, microbiological evaluation, and serological testing is often required for diagnosis.
Case Report
Patient History
A 58-year-old male presented to the respiratory medicine outpatient department with complaints of:
• Persistent cough for four months
• Intermittent hemoptysis for six weeks
• Low-grade fever
• Progressive weight loss
• Generalized fatigue
The patient reported occasional episodes of blood-streaked sputum that gradually increased in frequency. He also complained of reduced appetite and mild exertional breathlessness.
Past medical history revealed:
• Type 2 diabetes mellitus for 12 years
• Poor glycemic control
• Pulmonary tuberculosis treated successfully eight years earlier
There was no history of:
• Recent hospitalization
• Immunosuppressive therapy
• Malignancy
• HIV infection
• Smoking
Family history was unremarkable.
Clinical Examination
General examination revealed:
• Mild pallor
• Body mass index of 21 kg/m²
• No cyanosis
• No clubbing
Vital signs were stable:
• Blood pressure: 130/82 mmHg
• Pulse rate: 88 beats/minute
• Respiratory rate: 18 breaths/minute
• Temperature: 37.8°C
Respiratory examination demonstrated:
• Reduced air entry in the right upper lung zone
• Occasional coarse crackles
• No wheezing
Cardiovascular and abdominal examinations were unremarkable.
Clinical Evaluation
Differential Diagnosis
The following differential diagnoses were considered:
• Chronic pulmonary aspergillosis
• Reactivation tuberculosis
• Lung abscess
• Bronchiectasis
• Pulmonary malignancy
• Fungal pneumonia
The history of previous tuberculosis and hemoptysis raised suspicion for aspergilloma developing within a residual pulmonary cavity.
Investigations
Laboratory Evaluation
Routine laboratory investigations showed:
• Hemoglobin: 11.8 g/dL
• White blood cell count: 8,900/mm³
• Platelet count: 280,000/mm³
• ESR: 42 mm/hr
• C-reactive protein: Elevated
• HbA1c: 9.2%
• Renal function tests: Normal
• Liver function tests: Normal
HIV serology was negative.
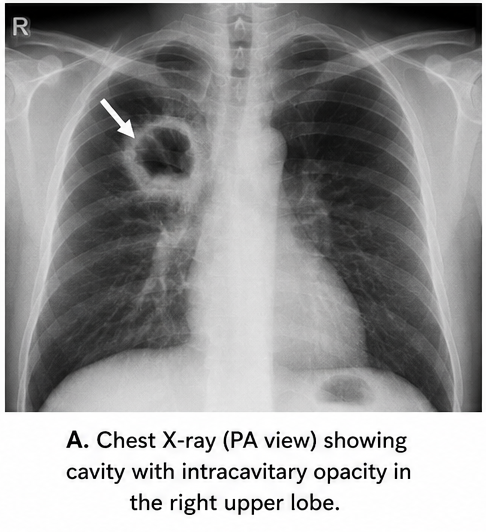
Chest Radiography
Chest X-ray revealed:
• Thick-walled cavity in the right upper lobe
• Intracavitary opacity
• Surrounding fibrotic changes
The findings warranted further imaging evaluation.
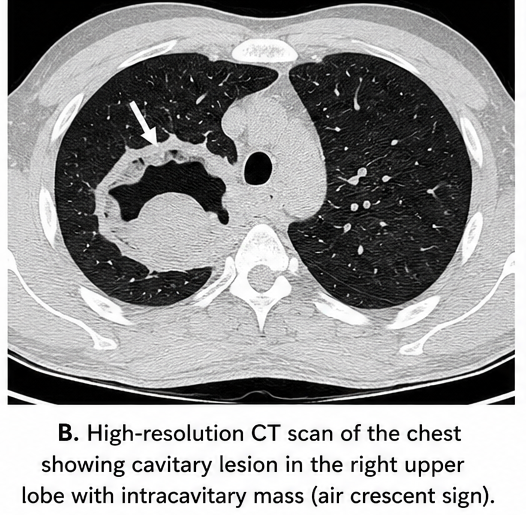
Computed Tomography
High-resolution CT scan demonstrated:
• A 4.5 cm cavitary lesion in the right upper lobe
• Rounded soft tissue density within the cavity
• Air crescent surrounding the intracavitary mass
• Adjacent fibrosis and pleural thickening
• No mediastinal lymphadenopathy
The imaging appearance was highly suggestive of pulmonary aspergilloma.
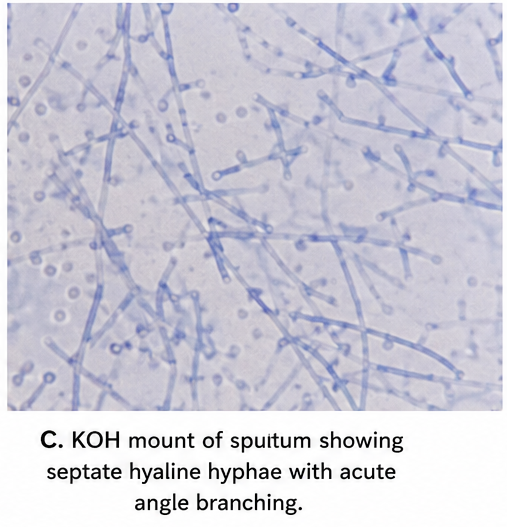
Microbiological Evaluation
Sputum samples were obtained for analysis.
Results showed:
• Negative acid-fast bacilli smear
• Negative GeneXpert for tuberculosis
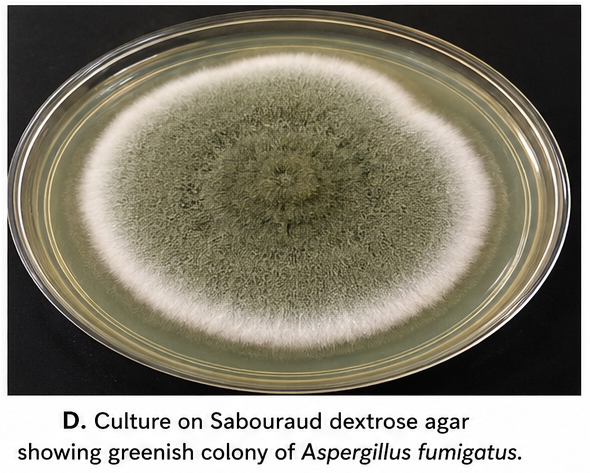
• Fungal culture positive for Aspergillus fumigatus
• No bacterial pathogens isolated
Serological Testing
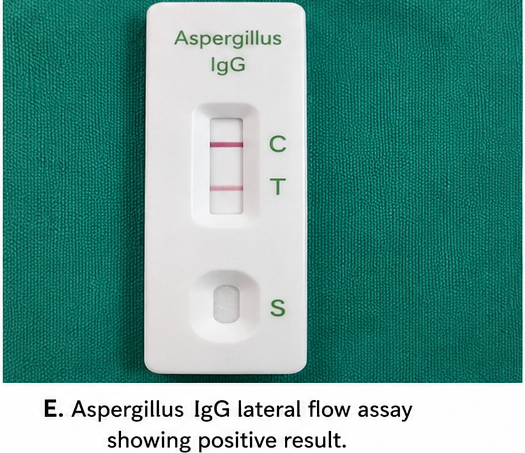
Serum Aspergillus IgG antibodies were significantly elevated.
Galactomannan assay demonstrated positive results, supporting active aspergillus infection.
Diagnosis
Based on clinical presentation, radiological findings, fungal culture, and serological evidence, a diagnosis of: Chronic Pulmonary Aspergillosis with Aspergilloma Formation was established.
Management and Outcome
Medical Treatment
Considering the patient's stable condition and absence of massive hemoptysis, conservative antifungal management was initiated.
The patient received:
• Oral voriconazole 200 mg twice daily
• Glycemic optimization
• Nutritional support
• Regular monitoring of liver function
The patient was counseled regarding treatment adherence and potential adverse effects.
Follow-Up
At 6 Weeks
Clinical improvement was observed:
• Reduction in cough
• No further hemoptysis
• Improved appetite
• Weight gain of 2 kg
Laboratory investigations demonstrated reduced inflammatory markers.
At 3 Months
The patient reported:
• Marked symptomatic improvement
• Resolution of fever
• Improved exercise tolerance
Repeat CT imaging showed:
• Reduction in cavity wall thickness
• Decreased inflammatory changes
• Stable fungal ball
At 6 Months
Further improvement was documented:
• No recurrent hemoptysis
• Normal daily activities restored
• Improved glycemic control
Radiological findings remained stable without progression.
Discussion
Pulmonary aspergillosis remains an important cause of chronic respiratory morbidity worldwide, particularly in patients with pre-existing lung disease. Tuberculosis-related cavities provide a favorable environment for colonization by Aspergillus species, resulting in aspergilloma formation.
Pathogenesis
The disease develops following inhalation of fungal conidia. In healthy individuals, alveolar macrophages and neutrophils eliminate inhaled spores efficiently. However, impaired immunity or abnormal lung architecture permits fungal proliferation and tissue colonization.
Chronic pulmonary aspergillosis is characterized by:
• Progressive cavitary destruction
• Chronic inflammation
• Fungal colonization
• Fibrosis
The intracavitary fungal ball consists of:
• Fungal hyphae
• Fibrin
• Inflammatory debris
• Necrotic tissue
Clinical Features
Patients commonly present with:
• Chronic cough
• Hemoptysis
• Weight loss
• Fatigue
• Dyspnea
• Fever
Hemoptysis is considered one of the most significant manifestations and may occasionally become life-threatening.
Diagnostic Evaluation
Diagnosis requires integration of:
• Clinical symptoms
• Radiological findings
• Serological evidence
• Microbiological confirmation
Chest CT remains the imaging modality of choice because it accurately demonstrates cavitary lesions, fungal balls, and associated complications.
Serum Aspergillus IgG testing has emerged as a valuable diagnostic tool for chronic pulmonary aspergillosis.
Treatment
Management depends on disease severity and patient characteristics.
Available treatment options include:
• Oral triazole antifungals
• Surgical resection
• Bronchial artery embolization for severe hemoptysis
• Long-term monitoring
Voriconazole and itraconazole are considered first-line therapies for chronic pulmonary aspergillosis.
Surgery may be indicated in:
• Massive hemoptysis
• Localized disease
• Failure of medical therapy
Complications
Potential complications include:
• Massive hemoptysis
• Respiratory failure
• Progressive pulmonary fibrosis
• Secondary bacterial infection
• Invasive aspergillosis
Early diagnosis significantly reduces morbidity and improves quality of life.
Prognosis
The prognosis depends on:
• Underlying lung disease
• Immune status
• Extent of pulmonary involvement
• Timeliness of treatment
Patients receiving appropriate antifungal therapy generally demonstrate symptom improvement and stabilization of radiological disease.
Conclusion
Pulmonary aspergillosis is an important opportunistic fungal infection that should be considered in patients with chronic respiratory symptoms, especially those with previous pulmonary tuberculosis or diabetes mellitus. This case illustrates the typical presentation of chronic pulmonary aspergillosis with aspergilloma formation and emphasizes the role of imaging, microbiological testing, and serological evaluation in establishing the diagnosis. Early recognition and prompt antifungal treatment can lead to significant clinical improvement, prevent complications, and enhance long-term outcomes.
References
- Denning DW, Cadranel J, Beigelman-Aubry C, Ader F, Chakrabarti A, Blot S, et al. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management. European Respiratory Journal. 2016;47(1):45-68. https://pubmed.ncbi.nlm.nih.gov/26699723/
- Patterson TF, Thompson GR III, Denning DW, Fishman JA, Hadley S, Herbrecht R, et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clinical Infectious Diseases. 2016;63(4):e1-e60. https://pubmed.ncbi.nlm.nih.gov/27365388/
- Kosmidis C, Denning DW. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015;70(3):270-277. https://pubmed.ncbi.nlm.nih.gov/25354514/
- Kousha M, Tadi R, Soubani AO. Pulmonary aspergillosis: a clinical review. European Respiratory Review. 2011;20(121):156-174. https://pubmed.ncbi.nlm.nih.gov/21881144/
- Latgé JP, Chamilos G. Aspergillus fumigatus and aspergillosis in 2019. Clinical Microbiology Reviews. 2020;33(1):e00140-18. https://pubmed.ncbi.nlm.nih.gov/31722887/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge