Plaque Psoriasis in an Adult Male Presenting with Chronic Scaly Skin Lesions – A Case Report
OthersPage Navigation
Abstract
Psoriasis is a chronic, immune-mediated inflammatory skin disorder characterized by erythematous, well-demarcated plaques covered with silvery-white scales. It affects approximately 2–3% of the global population and significantly impacts quality of life due to its chronic relapsing nature and associated comorbidities. Plaque psoriasis is the most common clinical subtype, accounting for nearly 80–90% of cases. Genetic predisposition, environmental triggers, infections, stress, obesity, smoking, and alcohol consumption contribute to disease development and exacerbation.
We report the case of a 42-year-old man who presented with chronic itchy scaly lesions over the elbows, knees, scalp, and lower back for eight months. Clinical examination and histopathological findings confirmed the diagnosis of chronic plaque psoriasis. The patient was treated with topical corticosteroids, vitamin D analogs, emollients, lifestyle modifications, and phototherapy, resulting in significant clinical improvement. This case highlights the importance of early diagnosis and comprehensive management of psoriasis to improve symptoms, prevent complications, and enhance quality of life.
Introduction
Psoriasis is a chronic inflammatory skin disease resulting from dysregulated interactions between the innate and adaptive immune systems. The disease is characterized by hyperproliferation of keratinocytes and increased inflammatory cytokine production, particularly involving the IL-23/Th17 pathway.
The condition may occur at any age but most commonly develops between 20 and 50 years of age. Plaque psoriasis is the predominant clinical variant and typically presents with erythematous plaques covered by silvery scales on extensor surfaces and the scalp.
Risk factors include:
• Family history of psoriasis
• Emotional stress
• Obesity
• Smoking
• Alcohol consumption
• Streptococcal infections
• Certain medications
Common clinical manifestations include:
• Well-defined erythematous plaques
• Silvery-white scales
• Pruritus
• Scalp involvement
• Nail abnormalities
• Symmetrical distribution
• Chronic relapsing course
Early diagnosis and appropriate treatment are essential to control symptoms and minimize disease burden.
Case Report
Patient History
A 42-year-old male presented to the dermatology outpatient department with complaints of:
• Itchy scaly skin lesions for eight months
• Progressive enlargement of plaques
• Intermittent burning sensation
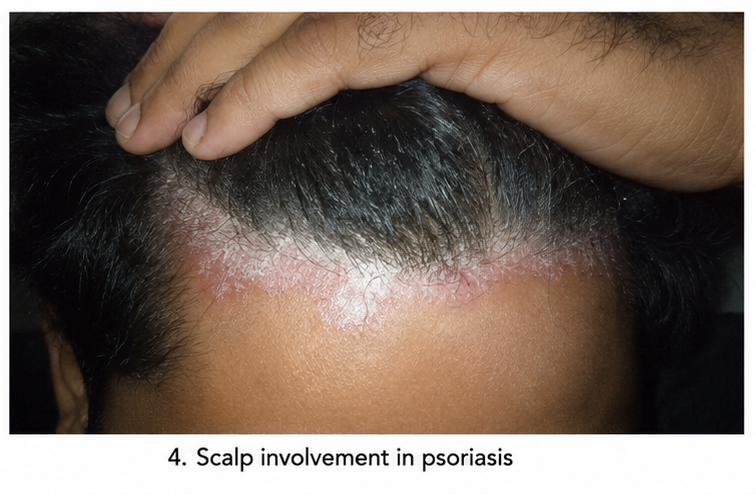
• Excessive scaling from the scalp
The lesions initially appeared over both elbows

and gradually spread to involve the
- knees,

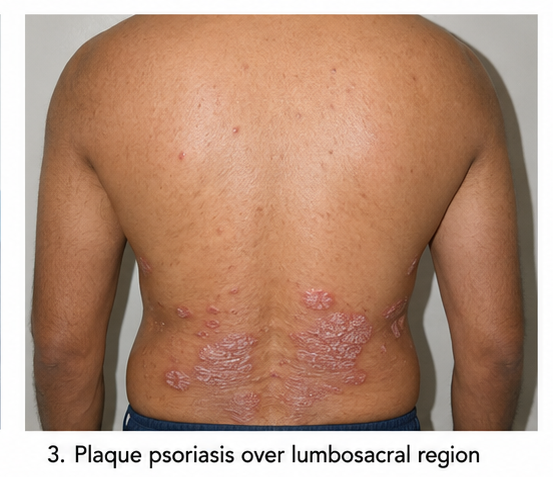
- lumbosacral region, and
- scalp
The patient reported worsening of symptoms during periods of psychological stress and winter months.
Past medical history was significant for:
• Mild hypertension controlled with medication
There was no history of:
• Diabetes mellitus
• Autoimmune disorders
• Tuberculosis
• Chronic liver disease
• HIV infection
Family history revealed that the patient’s father had similar skin lesions diagnosed as psoriasis.
Clinical Examination
General examination revealed:
• Conscious and oriented patient
• Body mass index: 29 kg/m²
• No pallor, cyanosis, or edema
Vital signs were stable:
• Pulse rate: 82 beats/minute
• Blood pressure: 132/84 mmHg
• Respiratory rate: 18 breaths/minute
• Temperature: Afebrile
Dermatological examination showed:
• Multiple well-demarcated erythematous plaques
• Thick silvery-white scales
• Bilateral involvement of elbows and knees
• Scalp plaques extending beyond the hairline
• Lumbosacral plaque involvement
Auspitz sign was positive, demonstrating pinpoint bleeding following scale removal.
Nail examination revealed:
• Mild nail pitting
• Longitudinal ridging
No evidence of joint swelling or tenderness was observed.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Chronic plaque psoriasis
• Seborrheic dermatitis
• Atopic dermatitis
• Lichen simplex chronicus
• Tinea corporis
• Pityriasis rubra pilaris
Investigations
Laboratory Evaluation
Routine investigations revealed:
• Hemoglobin: 13.9 g/dL
• White blood cell count: 7,400/mm³
• Platelet count: 278,000/mm³
• ESR: Mildly elevated
• C-reactive protein: Mildly elevated
Liver and renal function tests were within normal limits.
Radiological Evaluation
No radiological abnormalities were identified.
Histopathological Evaluation
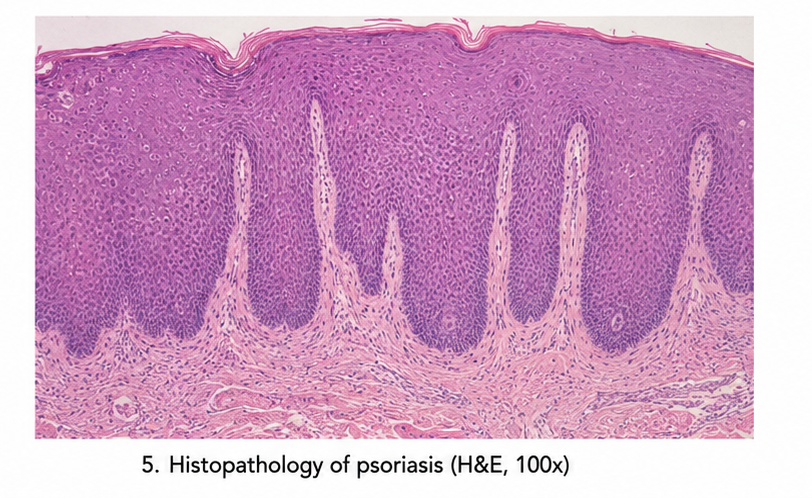
Skin biopsy from an elbow plaque demonstrated:
• Hyperkeratosis
• Parakeratosis
• Acanthosis
• Elongated rete ridges
• Dilated dermal capillaries
• Neutrophilic microabscesses
These findings were consistent with psoriasis vulgaris.
Diagnosis
Based on clinical presentation, examination findings, and histopathological confirmation, a diagnosis of: Chronic Plaque Psoriasis (Psoriasis Vulgaris) was established.
Management and Outcome
Medical Treatment
The patient was initiated on:
• Topical calcipotriol ointment
• Topical corticosteroid therapy
• Regular emollient application
• Medicated anti-psoriatic shampoo
• Narrowband ultraviolet B (NB-UVB) phototherapy
Lifestyle recommendations included:
• Weight reduction
• Smoking avoidance
• Stress management
• Regular skin moisturization
Follow-Up
At 4 Weeks
Clinical assessment revealed:
• Reduced scaling
• Improvement in itching
• Better skin hydration
At 8 Weeks
Significant improvement was noted:
• Reduction in plaque thickness
• Decreased erythema
• Improved cosmetic appearance
At 12 Weeks
Further improvement included:
• Marked reduction in lesion size
• Resolution of scalp scaling
• Improved quality of life
• No new lesions
The patient reported improved self-confidence and daily functioning.
Discussion
Psoriasis is a chronic immune-mediated disease affecting the skin, nails, and joints. The pathogenesis involves activation of dendritic cells and T lymphocytes, leading to excessive production of inflammatory cytokines such as TNF-α, IL-17, and IL-23.
Clinical Features
Plaque psoriasis commonly presents with:
• Erythematous plaques
• Silvery scales
• Symmetrical distribution
• Pruritus
• Scalp involvement
• Nail changes
The disease may also be associated with:
• Psoriatic arthritis
• Cardiovascular disease
• Metabolic syndrome
• Obesity
• Depression and anxiety
Diagnostic Evaluation
Diagnosis is primarily clinical but may be supported by skin biopsy in atypical cases.
Characteristic findings include:
• Well-defined plaques
• Positive Auspitz sign
• Nail pitting
• Histological evidence of epidermal hyperplasia and inflammation
Treatment
Management depends on disease severity and extent.
Therapeutic options include:
• Topical corticosteroids
• Vitamin D analogs
• Emollients
• Phototherapy
• Methotrexate
• Cyclosporine
• Biologic therapies
Modern biologic agents targeting IL-17 and IL-23 pathways have significantly improved outcomes in moderate-to-severe disease.
Prevention
Although psoriasis cannot be prevented completely, disease flares may be minimized through:
• Stress reduction
• Weight management
• Smoking cessation
• Limiting alcohol intake
• Avoiding known triggers
• Adherence to prescribed therapy
Prognosis
Psoriasis is a lifelong chronic inflammatory skin disorder characterized by periods of remission and relapse. Although there is currently no definitive cure, most patients can achieve satisfactory disease control through appropriate medical treatment, lifestyle modifications, and regular follow-up. The clinical course varies among individuals, with some experiencing infrequent mild flare-ups while others may develop persistent or extensive disease requiring long-term therapy. Early diagnosis and timely initiation of treatment play a crucial role in reducing disease severity, minimizing skin damage, and preventing complications such as psoriatic arthritis and metabolic comorbidities. Effective management not only improves physical symptoms such as scaling, erythema, and pruritus but also enhances psychological well-being and overall quality of life. Continuous patient education, adherence to treatment, and avoidance of known triggers are essential for maintaining prolonged remission and reducing the risk of recurrent flare-ups and psychosocial distress.
Conclusion
Plaque psoriasis is a common chronic inflammatory skin disorder that significantly impacts physical, emotional, and social well-being. This case highlights the classical presentation of psoriasis with erythematous scaly plaques involving the elbows, knees, scalp, and lower back. Early diagnosis, appropriate topical therapy, phototherapy, and lifestyle modification resulted in substantial clinical improvement and enhanced quality of life. Continuous patient education and long-term follow-up remain essential for effective disease management.
References
- Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301-1315. https://pubmed.ncbi.nlm.nih.gov/33812489/
- Armstrong AW, Read C. Pathophysiology, Clinical Presentation, and Treatment of Psoriasis: A Review. JAMA. 2020;323(19):1945-1960. https://pubmed.ncbi.nlm.nih.gov/32427307/
- Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386(9997):983-994. https://pubmed.ncbi.nlm.nih.gov/26025581/
- Rendon A, Schäkel K. Psoriasis Pathogenesis and Treatment. Int J Mol Sci. 2019;20(6):1475. https://pubmed.ncbi.nlm.nih.gov/30909615/
- Kamiya K, Kishimoto M, Sugai J, Komine M, Ohtsuki M. Risk Factors for the Development of Psoriasis. Int J Mol Sci. 2019;20(18):4347. https://pubmed.ncbi.nlm.nih.gov/31487734/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge