Goitre: Clinical Presentation, Diagnostic Evaluation, Surgical Management, and Outcome – A Case Report
OthersPage Navigation
Abstract
Goitre refers to the abnormal enlargement of the thyroid gland and remains one of the most common endocrine disorders worldwide. Although iodine deficiency remains a major cause globally, goitre may also develop due to autoimmune diseases, nodular thyroid disease, genetic predisposition, inflammatory conditions, and thyroid neoplasms. Patients may present with a visible neck swelling, compressive symptoms, cosmetic concerns, or thyroid dysfunction.
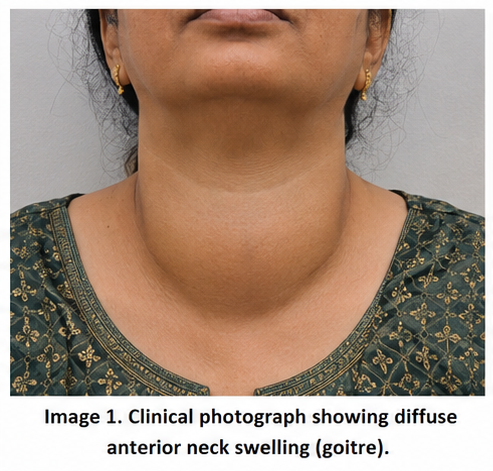
We present the case of a 45-year-old female who presented with progressive anterior neck swelling associated with difficulty swallowing and a sensation of neck fullness. Clinical examination revealed a diffuse thyroid enlargement. Thyroid function tests demonstrated euthyroid status, while ultrasonography identified a multinodular goitre. Fine-needle aspiration cytology excluded malignancy. Due to progressive compressive symptoms and cosmetic concerns, the patient underwent total thyroidectomy with an excellent postoperative outcome.
This case highlights the importance of comprehensive clinical assessment, appropriate imaging, cytological evaluation, and timely surgical intervention in the management of multinodular goitre.
Introduction
Goitre is defined as enlargement of the thyroid gland beyond its normal size. The thyroid gland plays a critical role in regulating metabolism, growth, and development through the secretion of thyroid hormones.
The causes of goitre are diverse and include:
• Iodine deficiency
• Multinodular thyroid disease
• Graves’ disease
• Hashimoto thyroiditis
• Thyroid adenoma
• Thyroid carcinoma
• Genetic and environmental factors
Goitre may be classified as:
• Diffuse goitre
• Nodular goitre
• Multinodular goitre
• Toxic goitre
• Non-toxic goitre
Although many patients remain asymptomatic, progressive enlargement may lead to dysphagia, dyspnea, hoarseness, and significant cosmetic concerns. Early diagnosis is important to identify underlying pathology and prevent complications.
Case Report
Patient History
A 45-year-old female presented to the outpatient department with complaints of:
• Progressive swelling in the front of the neck for 2 years
• Difficulty swallowing solid food for 3 months
• Sensation of pressure in the neck
• Mild discomfort while lying flat
The swelling had gradually increased in size over time.
The patient denied:
• Fever
• Weight loss
• Neck pain
• Palpitations
• Excessive sweating
• Tremors
There was no history of:
• Radiation exposure
• Thyroid surgery
• Family history of thyroid cancer
Past medical history was unremarkable.
Clinical Examination
General Examination
• Blood pressure: 128/82 mmHg
• Pulse rate: 78/min
• Respiratory rate: 18/min
• Temperature: Afebrile
• Oxygen saturation: 99% on room air
The patient appeared comfortable with no signs of thyrotoxicosis or hypothyroidism.
Local Examination
Inspection revealed:
• Diffuse enlargement of the anterior neck
• Symmetrical thyroid swelling
• Visible movement with deglutition
• No overlying skin changes
Palpation demonstrated:
• Enlarged thyroid gland involving both lobes
• Multiple palpable nodules
• Firm consistency
• Non-tender swelling
• No local warmth
No cervical lymphadenopathy was detected.
Pemberton’s sign was negative.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Multinodular goitre
• Colloid goitre
• Thyroid adenoma
• Hashimoto thyroiditis
• Thyroid malignancy
• Graves’ disease
The gradual progression and multinodular nature of the swelling favored multinodular goitre.
Investigations
Laboratory Evaluation
Routine investigations revealed:
• Hemoglobin: 12.6 g/dL
• Total leukocyte count: 7,400/mm³
• Platelet count: 258,000/mm³
• Blood glucose: Normal
• Renal function tests: Normal
• Liver function tests: Normal
Thyroid Function Tests
Results demonstrated:
• TSH: 2.4 mIU/L
• Free T3: Normal
• Free T4: Normal
These findings confirmed euthyroid status.
Thyroid Ultrasonography
Ultrasound examination revealed:
• Enlarged thyroid gland
• Multiple bilateral thyroid nodules
• Largest nodule measuring 3.2 cm
• Mixed cystic and solid components
• Increased gland volume
• No suspicious cervical lymph nodes
Findings were suggestive of multinodular goitre.

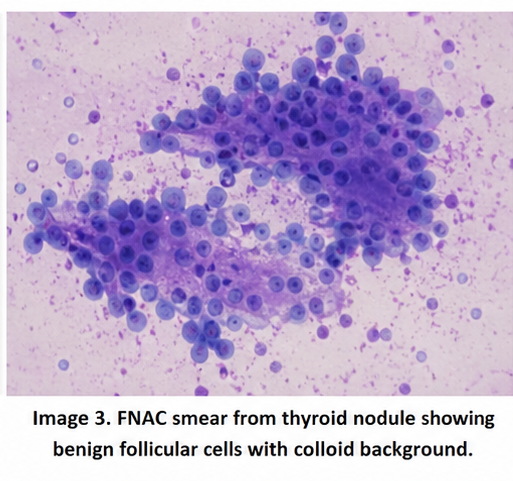
Fine-Needle Aspiration Cytology
FNAC was performed from the dominant nodule.
Cytological findings revealed:
• Benign follicular cells
• Colloid-rich background
• No atypia
• No evidence of malignancy
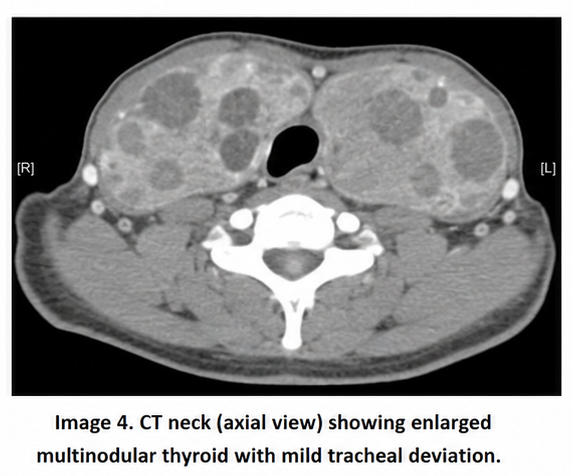
Computed Tomography Scan
CT neck demonstrated:
• Enlarged multinodular thyroid gland
• Mild tracheal deviation
• No retrosternal extension
• Mild compression of surrounding structures
Diagnosis
Based on clinical examination, imaging, and cytological findings, a diagnosis of: Benign Multinodular Euthyroid Goitre with Compressive Symptoms was established.
Management and Outcome
Initial Management
The patient was counseled regarding available treatment options.
Management considerations included:
• Observation
• Thyroid hormone suppression therapy
• Radioiodine therapy
• Surgical intervention
Because of progressive enlargement, dysphagia, and tracheal deviation, surgery was recommended.
Surgical Management
The patient underwent:
Total Thyroidectomy
Intraoperative findings included:
• Enlarged multinodular thyroid gland
• No invasion of adjacent structures
• Preservation of recurrent laryngeal nerves
• Preservation of parathyroid glands
The surgery was completed without complications.
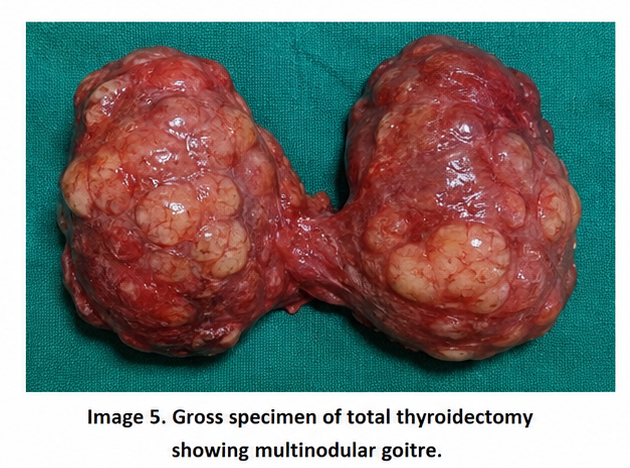
Histopathological Examination
Microscopic examination demonstrated:
• Multinodular hyperplasia
• Colloid-filled follicles
• No malignancy
The diagnosis of benign multinodular goitre was confirmed.
Postoperative Course
At 1 Week
• Minimal pain
• Normal wound healing
• No voice changes
• No hypocalcemia
At 1 Month
• Complete resolution of swallowing difficulty
• Excellent cosmetic outcome
• Stable thyroid hormone replacement therapy
At 6 Months
• No recurrence
• Normal quality of life
• Well-controlled thyroid hormone levels
Discussion
Pathophysiology
Goitre develops due to enlargement of thyroid follicular cells resulting from chronic stimulation of the gland.
Mechanisms include:
• Increased TSH stimulation
• Iodine deficiency
• Autoimmune activation
• Genetic susceptibility
• Growth factor-mediated cellular proliferation
Repeated cycles of stimulation and involution may lead to nodular transformation and multinodular goitre formation.
Epidemiology
Important epidemiological features include:
• More common in women
• Increased prevalence with age
• Higher incidence in iodine-deficient regions
• One of the most common endocrine disorders worldwide
• Significant healthcare burden in developing countries
Although iodine supplementation has reduced prevalence in many regions, multinodular goitre remains common.
Clinical Manifestations
Patients may present with:
• Neck swelling
• Cosmetic concerns
• Dysphagia
• Dyspnea
• Hoarseness
• Neck discomfort
Large goitres may produce compressive symptoms due to pressure on adjacent structures.
Some patients may develop:
• Hyperthyroidism
• Hypothyroidism
• Retrosternal extension
• Tracheal compression
Diagnostic Considerations
Diagnosis is based on:
- Detailed clinical history
- Physical examination
- Thyroid function tests
- Ultrasonography
- Fine-needle aspiration cytology
- Cross-sectional imaging when indicated
Ultrasonography remains the primary imaging modality for thyroid evaluation.
FNAC plays a critical role in excluding malignancy and guiding management decisions.
Treatment Modalities
Observation
Suitable for:
• Small asymptomatic goitres
• Stable thyroid nodules
Medical Therapy
May include:
• Thyroid hormone replacement
• Treatment of thyroid dysfunction
However, medical therapy has limited effectiveness in reducing large multinodular goitres.
Radioiodine Therapy
Useful in selected patients with:
• Toxic multinodular goitre
• Surgical contraindications
Surgical Intervention
Indications include:
• Compressive symptoms
• Cosmetic deformity
• Suspicion of malignancy
• Retrosternal extension
• Large goitre size
Total thyroidectomy provides definitive treatment in appropriately selected patients.
Complications
Potential complications of untreated goitre include:
• Airway compression
• Dysphagia
• Hyperthyroidism
• Hemorrhage into nodules
• Cosmetic disfigurement
• Rare malignant transformation
Early evaluation and treatment reduce the risk of these complications.
Prognosis
The prognosis depends upon:
• Underlying etiology
• Presence of malignancy
• Size of the gland
• Thyroid function status
• Timeliness of treatment
Most patients with benign multinodular goitre experience excellent outcomes following definitive treatment.
Conclusion
Goitre remains a common endocrine disorder with diverse etiologies and clinical presentations. Careful clinical assessment combined with thyroid function testing, ultrasonography, and cytological evaluation enables accurate diagnosis and appropriate treatment planning. This case demonstrates the successful management of benign multinodular goitre presenting with compressive symptoms through timely surgical intervention and postoperative thyroid hormone replacement. Early recognition, individualized treatment, and long-term follow-up remain essential for preventing complications and ensuring favorable patient outcomes.
References
- Hegedüs L. Clinical practice. The thyroid nodule. N Engl J Med. 2004;351(17):1764-1771. PMID: 15496625.https://pubmed.ncbi.nlm.nih.gov/15496625/
- Durante C, Grani G, Lamartina L, Filetti S, Mandel SJ, Cooper DS. The diagnosis and management of thyroid nodules. JAMA. 2018;319(9):914-924. PMID: 29509871. https://pubmed.ncbi.nlm.nih.gov/29509871/
- Gharib H, Papini E, Garber JR, et al. American Association of Clinical Endocrinologists guidelines for management of thyroid nodules. Endocr Pract. 2016;22(5):622-639. PMID: 27167915. https://pubmed.ncbi.nlm.nih.gov/27167915/
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1-133. PMID: 26462967. https://pubmed.ncbi.nlm.nih.gov/26462967/
- Dean DS, Gharib H. Epidemiology of thyroid nodules. Best Pract Res Clin Endocrinol Metab. 2008;22(6):901-911. PMID: 19041821. https://pubmed.ncbi.nlm.nih.gov/19041821/
- Brito JP, Gionfriddo MR, Al Nofal A, et al. The accuracy of thyroid nodule ultrasound to predict thyroid cancer. J Clin Endocrinol Metab. 2014;99(4):1253-1263. PMID: 24423338. https://pubmed.ncbi.nlm.nih.gov/24423338/
- Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167-1214. PMID: 19860577. https://pubmed.ncbi.nlm.nih.gov/19860577/
- Paschke R, Hegedüs L, Alexander E, Valcavi R, Papini E, Gharib H. Thyroid nodule guidelines: agreement, disagreement and need for future research. Nat Rev Endocrinol. 2011;7(6):354-361. PMID: 21468021. https://pubmed.ncbi.nlm.nih.gov/21468021/
- Guth S, Theune U, Aberle J, Galach A, Bamberger CM. Very high prevalence of thyroid nodules detected by high-frequency ultrasound examination. Eur J Clin Invest. 2009;39(8):699-706. PMID: 19508352. https://pubmed.ncbi.nlm.nih.gov/19508352/
- Hegedüs L, Bonnema SJ, Bennedbæk FN. Management of simple nodular goiter: current status and future perspectives. Endocr Rev. 2003;24(1):102-132. PMID: 12588810. https://pubmed.ncbi.nlm.nih.gov/12588810/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge