Acute Urticaria Following Food Allergy in a Young Adult Successfully Managed with Antihistamines – A Case Report
OthersPage Navigation
Abstract
Urticaria is a common dermatological condition characterized by the sudden appearance of transient, pruritic wheals with or without angioedema. It affects approximately 15–25% of individuals at least once during their lifetime and is commonly triggered by infections, foods, medications, insect bites, or environmental factors. Acute urticaria lasts for less than six weeks and is primarily mediated by mast cell degranulation with subsequent histamine release. Although most episodes are self-limiting, severe cases may progress to angioedema or anaphylaxis, requiring prompt recognition and treatment. Early diagnosis based on clinical history and exclusion of differential diagnoses facilitates appropriate management and prevents recurrence.
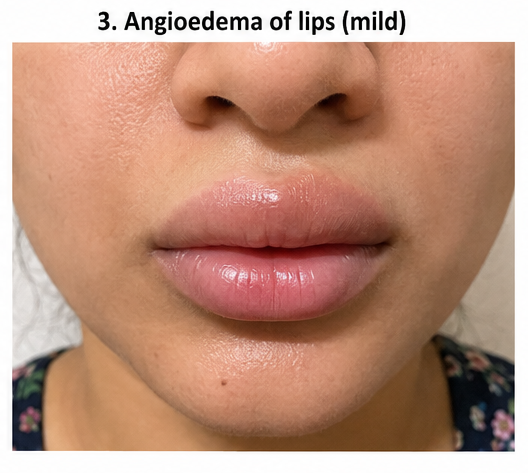
We report the case of a 28-year-old woman who presented with sudden-onset intensely itchy erythematous wheals over the trunk and extremities accompanied by mild swelling of the lips after consuming shellfish. Clinical examination and laboratory investigations supported the diagnosis of acute food-induced urticaria without systemic anaphylaxis. The patient was successfully treated with oral second-generation antihistamines, a short course of corticosteroids, avoidance of the offending allergen, and patient education. Complete resolution of symptoms occurred within five days without recurrence during follow-up. This case highlights the importance of early recognition, identification of triggering factors, and evidence-based treatment in achieving rapid symptom control.
Introduction
Urticaria is a vascular reaction of the skin characterized by transient wheals resulting from localized dermal edema caused by mast cell activation and release of histamine, leukotrienes, prostaglandins, and other inflammatory mediators. Individual wheals typically persist for less than 24 hours and resolve without residual pigmentation or scarring. The condition may occur alone or in association with angioedema involving the deeper dermis and subcutaneous tissues.
Acute urticaria accounts for the majority of urticaria cases and usually resolves within six weeks. Common precipitating factors include food allergens such as shellfish, peanuts, eggs, and milk; medications including antibiotics and non-steroidal anti-inflammatory drugs; viral infections; insect stings; and physical stimuli.
Clinical manifestations include:
- Sudden onset of intensely itchy wheals
- Erythematous raised plaques of varying size
- Migratory skin lesions
- Angioedema involving lips, eyelids, or face
- Occasionally abdominal pain or respiratory symptoms in severe allergic reactions
Although diagnosis is primarily clinical, careful evaluation is necessary to exclude anaphylaxis, urticarial vasculitis, autoimmune disorders, and other dermatological conditions. Second-generation H1-antihistamines remain the first-line therapy, while systemic corticosteroids are reserved for severe acute episodes.
Case Report
Patient History
A 28-year-old woman presented to the dermatology outpatient department with complaints of sudden-onset itchy skin rashes over the arms, trunk, neck, and thighs for six hours. The lesions appeared approximately one hour after consuming shellfish at a restaurant. She also noticed mild swelling of her lips but denied difficulty breathing, wheezing, throat tightness, dizziness, or loss of consciousness.
She had no previous history of chronic urticaria, asthma, eczema, autoimmune disease, or recent infections. There was no history of new medications or insect bites. Family history was unremarkable for allergic disorders.
Clinical Examination
The patient was alert and hemodynamically stable.
Vital signs
- Pulse rate: 84 beats/minute
- Blood pressure: 118/74 mmHg
- Respiratory rate: 18 breaths/minute
- Temperature: 98.4°F
- Oxygen saturation: 99% on room air
Dermatological examination
- Multiple erythematous, raised wheals of varying sizes distributed over the trunk, upper limbs, neck, and thighs
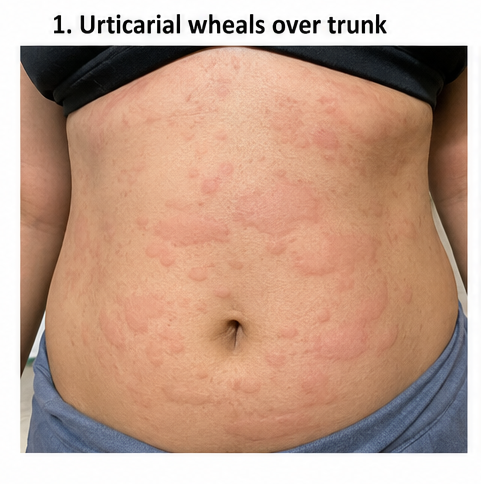

- Lesions showed a migratory pattern
- Mild edema of the upper lip
- No mucosal ulceration
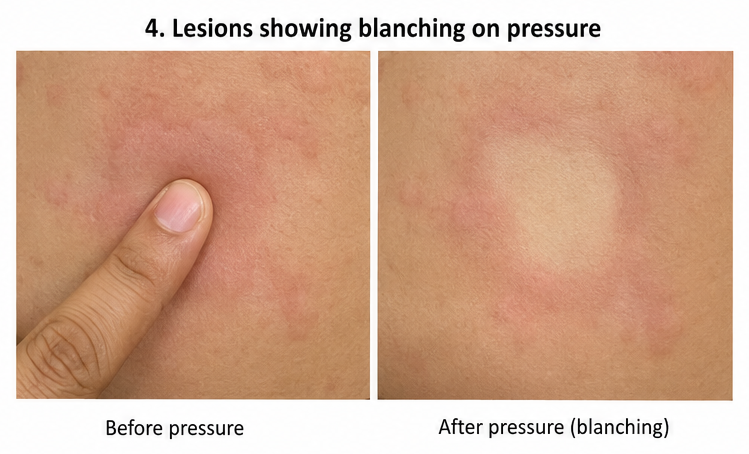
- Individual wheals were blanchable and intensely pruritic
- No purpura or residual pigmentation
Systemic examination
- Respiratory examination was normal with no wheeze or stridor.
- Cardiovascular and abdominal examinations were unremarkable.
Differential Diagnosis
The following conditions were considered:
- Acute allergic urticaria
- Drug-induced urticaria
- Viral exanthem
- Urticarial vasculitis
- Contact dermatitis
- Early anaphylaxis
Investigations
Routine laboratory investigations were performed to exclude systemic illness.
Laboratory Evaluation
- Hemoglobin: 13.2 g/dL
- Total leukocyte count: 8,900/mm³
- Platelet count: 284,000/mm³
- Absolute eosinophil count: 520 cells/µL (mildly elevated)
- C-reactive protein: Within normal limits
- Liver function tests: Normal
- Renal function tests: Normal
- Serum electrolytes: Normal
Serum tryptase estimation was not performed because the patient showed no evidence of systemic anaphylaxis.
Based on the temporal relationship between shellfish ingestion and symptom onset, allergy testing was deferred until complete symptom resolution.
Diagnosis
Considering the clinical presentation, physical examination, and history of recent shellfish consumption, a diagnosis of acute food-induced urticaria with mild angioedema was established.
Management and Outcome
The patient was immediately advised to avoid further exposure to shellfish.
Treatment included:
- Oral cetirizine 10 mg twice daily
- Oral prednisolone 30 mg once daily for three days
- Calamine lotion for symptomatic relief
- Adequate hydration
- Avoidance of alcohol, NSAIDs, and known food allergens
The patient was observed in the emergency department for four hours because of mild lip swelling. Throughout observation, she remained hemodynamically stable without progression to respiratory compromise or hypotension.
Since there were no features of anaphylaxis, intramuscular adrenaline was not required.
The itching reduced significantly within 24 hours, and the wheals gradually disappeared over the next three days.
Follow-Up
Three Days
- Marked reduction in itching
- Nearly complete disappearance of wheals
- Complete resolution of lip swelling
- No development of new lesions
One Week
- Complete clearance of skin lesions
- No residual pigmentation
- No recurrence of symptoms
- Oral corticosteroids discontinued
- Antihistamine continued for another week

One Month
The patient remained symptom-free and successfully avoided shellfish. She was counseled regarding recognition of severe allergic reactions and advised to undergo formal allergy evaluation for confirmation of the suspected food trigger.
Discussion
Acute urticaria is among the most frequent allergic skin disorders encountered in clinical practice. The disease results from activation of dermal mast cells and basophils, leading to the release of histamine and other inflammatory mediators that increase vascular permeability and produce characteristic wheals and pruritus.
Food allergy is an important cause of acute urticaria in adults, with shellfish being one of the most common triggers worldwide. Symptoms usually develop within minutes to a few hours after exposure. Diagnosis relies heavily on obtaining a detailed clinical history because routine laboratory investigations are frequently normal.
The principal objective of treatment is rapid symptom control while preventing progression to life-threatening anaphylaxis. International guidelines recommend second-generation H1-antihistamines as first-line therapy due to their excellent efficacy and favorable safety profile. Short courses of systemic corticosteroids may be considered in severe acute episodes associated with extensive skin involvement or angioedema but should not be used for prolonged periods because of potential adverse effects.
Recognition of warning signs such as hypotension, bronchospasm, laryngeal edema, or persistent gastrointestinal symptoms is essential, as these indicate evolving anaphylaxis requiring immediate intramuscular adrenaline. Fortunately, the present patient exhibited only mild angioedema without systemic involvement and responded promptly to conservative therapy.
Patient education remains a cornerstone of management. Identification and avoidance of precipitating allergens substantially reduce recurrence. Individuals with confirmed food allergies should be informed about careful food labeling, cross-contamination risks, and the importance of seeking urgent medical care if respiratory or cardiovascular symptoms develop following future exposures.
Prognosis
Acute urticaria generally has an excellent prognosis, with most patients achieving complete recovery within days to weeks following elimination of the offending trigger and appropriate antihistamine therapy. Recurrence can usually be prevented through allergen avoidance and patient education. Progression to chronic urticaria is uncommon after isolated food-induced episodes. Long-term outcomes are favorable when early recognition and evidence-based treatment are instituted.
Conclusion
Acute food-induced urticaria is a common hypersensitivity reaction that can cause considerable patient distress but usually responds rapidly to timely treatment. Careful clinical history, recognition of potential triggers, and exclusion of anaphylaxis are fundamental to diagnosis. Second-generation antihistamines remain the cornerstone of therapy, while short courses of corticosteroids may be beneficial in selected severe cases. Early intervention, allergen avoidance, and patient counseling are essential to minimize recurrence and improve quality of life.
References
- Zuberbier T, Abdul Latiff AH, Abuzakouk M, et al. The EAACI/GA²LEN/EuroGuiDerm/APAAACI Guideline for the Definition, Classification, Diagnosis and Management of Urticaria. Allergy. 2022;77(3):734–766. https://pubmed.ncbi.nlm.nih.gov/34536239/
- American Academy of Allergy, Asthma & Immunology. Acute and Chronic Urticaria Practice Resources. https://www.aaaai.org/
- Bernstein JA, Lang DM, Khan DA, et al. The Diagnosis and Management of Acute and Chronic Urticaria: 2014 Update. Journal of Allergy and Clinical Immunology. 2014;133(5):1270–1277. https://pubmed.ncbi.nlm.nih.gov/24766875/
- Kolkhir P, Giménez-Arnau AM, Kulthanan K, et al. Urticaria. Nature Reviews Disease Primers. 2022;8:61. https://pubmed.ncbi.nlm.nih.gov/36192669/
- Schaefer P. Acute and Chronic Urticaria: Evaluation and Treatment. American Family Physician. 2017;95(11):717–724. https://pubmed.ncbi.nlm.nih.gov/28671445/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge