Deep Vein Thrombosis: Clinical Presentation, Diagnostic Evaluation, Anticoagulant Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Deep vein thrombosis (DVT) is a common vascular disorder characterized by the formation of thrombi within the deep venous system, most frequently affecting the lower extremities. DVT represents a major component of venous thromboembolism (VTE) and is associated with significant morbidity and mortality due to complications such as pulmonary embolism and post-thrombotic syndrome.
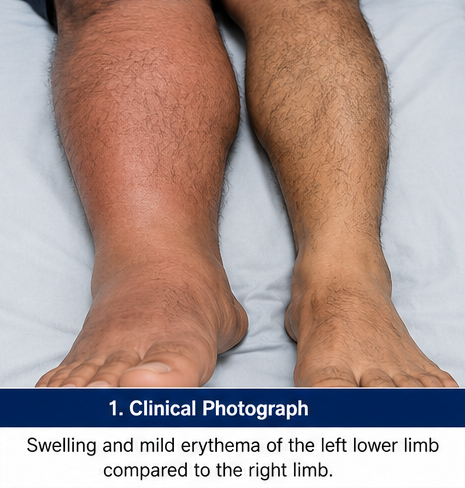
Patients typically present with unilateral limb swelling, pain, warmth, erythema, and tenderness. Early diagnosis using clinical assessment and imaging studies is essential to prevent life-threatening complications.
We present the case of a 58-year-old male who presented with progressive swelling and pain of the left lower limb following prolonged immobilization after orthopedic surgery. Duplex ultrasonography confirmed extensive thrombosis involving the femoral and popliteal veins. The patient was successfully treated with anticoagulation therapy and supportive measures, resulting in symptom resolution and prevention of thromboembolic complications.
This case highlights the importance of early recognition, prompt diagnostic evaluation, and evidence-based anticoagulant therapy in achieving favorable outcomes in patients with deep vein thrombosis.
Introduction
Deep vein thrombosis refers to the formation of a blood clot within the deep venous circulation, most commonly involving the veins of the lower extremities. It is a major healthcare concern worldwide and contributes significantly to cardiovascular morbidity and mortality.
The pathogenesis of DVT is classically explained by Virchow’s triad, which includes:
• Venous stasis
• Endothelial injury
• Hypercoagulability
Several risk factors predispose individuals to DVT, including:
• Advanced age
• Major surgery
• Trauma
• Prolonged immobilization
• Malignancy
• Obesity
• Pregnancy
• Hormonal therapy
• Inherited thrombophilia
Untreated DVT may progress to pulmonary embolism, chronic venous insufficiency, or post-thrombotic syndrome. Therefore, timely diagnosis and management are crucial.
Case Report
Patient History
A 58-year-old male presented to the emergency department with complaints of:
• Swelling of the left lower limb for 5 days
• Progressive calf pain
• Heaviness while walking
• Mild redness over the affected leg
The symptoms developed gradually and worsened over several days.
Further history revealed:
• Recent total knee replacement surgery performed 3 weeks earlier
• Reduced mobility during postoperative recovery
• No history of chest pain or breathlessness
Past medical history included:
• Hypertension for 10 years
• Obesity
• Dyslipidemia
There was no history of:
• Previous venous thromboembolism
• Active malignancy
• Smoking
• Known clotting disorders
Clinical Examination
General Examination
• Blood pressure: 136/84 mmHg
• Pulse rate: 88/min
• Respiratory rate: 18/min
• Temperature: Afebrile
• Oxygen saturation: 98% on room air
Local Examination
Inspection revealed:
• Diffuse swelling of the left lower limb
• Mild erythema over the calf region
• Increased circumference compared with the right leg
Palpation demonstrated:
• Local warmth
• Tenderness along the calf muscles
• Pitting edema extending up to the knee
Calf circumference measurement showed:
• Left calf: 42 cm
• Right calf: 37 cm
Peripheral pulses were palpable bilaterally.
No skin ulceration or gangrene was observed.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Deep vein thrombosis
• Cellulitis
• Ruptured Baker’s cyst
• Lymphedema
• Superficial thrombophlebitis
The recent surgery, immobilization, unilateral swelling, and calf tenderness strongly suggested DVT.
Investigations
Laboratory Evaluation
Routine investigations revealed:
• Hemoglobin: 13.8 g/dL
• Total leukocyte count: 8,200/mm³
• Platelet count: 245,000/mm³
• Serum creatinine: Normal
• Liver function tests: Normal
D-Dimer Assay
Laboratory testing demonstrated:
• Elevated D-dimer level: 2.8 μg/mL FEU
The elevated level supported the possibility of active thrombosis.
Compression Duplex Ultrasonography
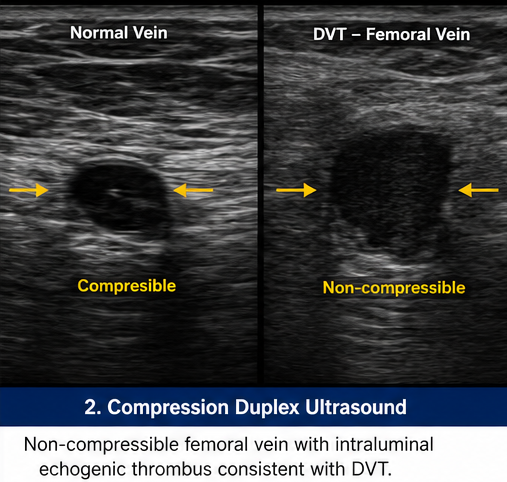
Ultrasound examination demonstrated:
• Non-compressible femoral vein
• Non-compressible popliteal vein
• Intraluminal echogenic thrombus
• Reduced venous flow
These findings confirmed acute deep vein thrombosis.
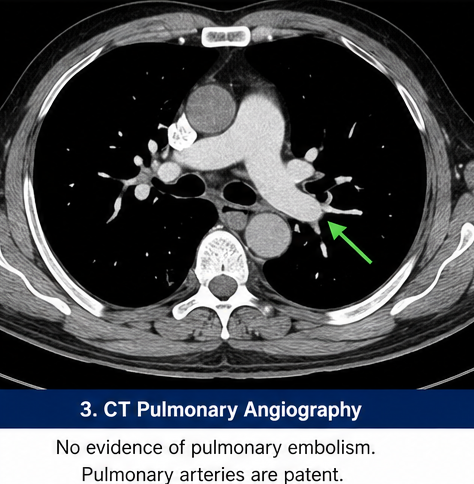
Computed Tomography Pulmonary Angiography (CTPA)
CTPA was performed to exclude pulmonary embolism and demonstrated:
• No evidence of pulmonary embolism
Thrombophilia Screening
Testing for inherited thrombophilia was deferred because the thrombotic event was provoked by recent surgery and immobilization.
Diagnosis
Based on clinical assessment and imaging findings, a diagnosis of: Acute Proximal Deep Vein Thrombosis of the Left Lower Limb was established.
Management and Outcome
Initial Management
The patient was admitted for anticoagulation therapy.
Treatment included:
• Low-molecular-weight heparin (LMWH)
• Transition to oral anticoagulation with apixaban
• Graduated compression stockings
• Limb elevation
• Early mobilization as tolerated

The patient was educated regarding:
• Medication adherence
• Recognition of bleeding complications
• Importance of follow-up
• Prevention of recurrent thrombosis
Follow-Up and Clinical Course
At 1 Week
• Reduction in calf pain
• Improved ambulation
• No bleeding complications
At 1 Month
• Significant reduction in limb swelling
• Improved quality of life
• Good compliance with anticoagulant therapy
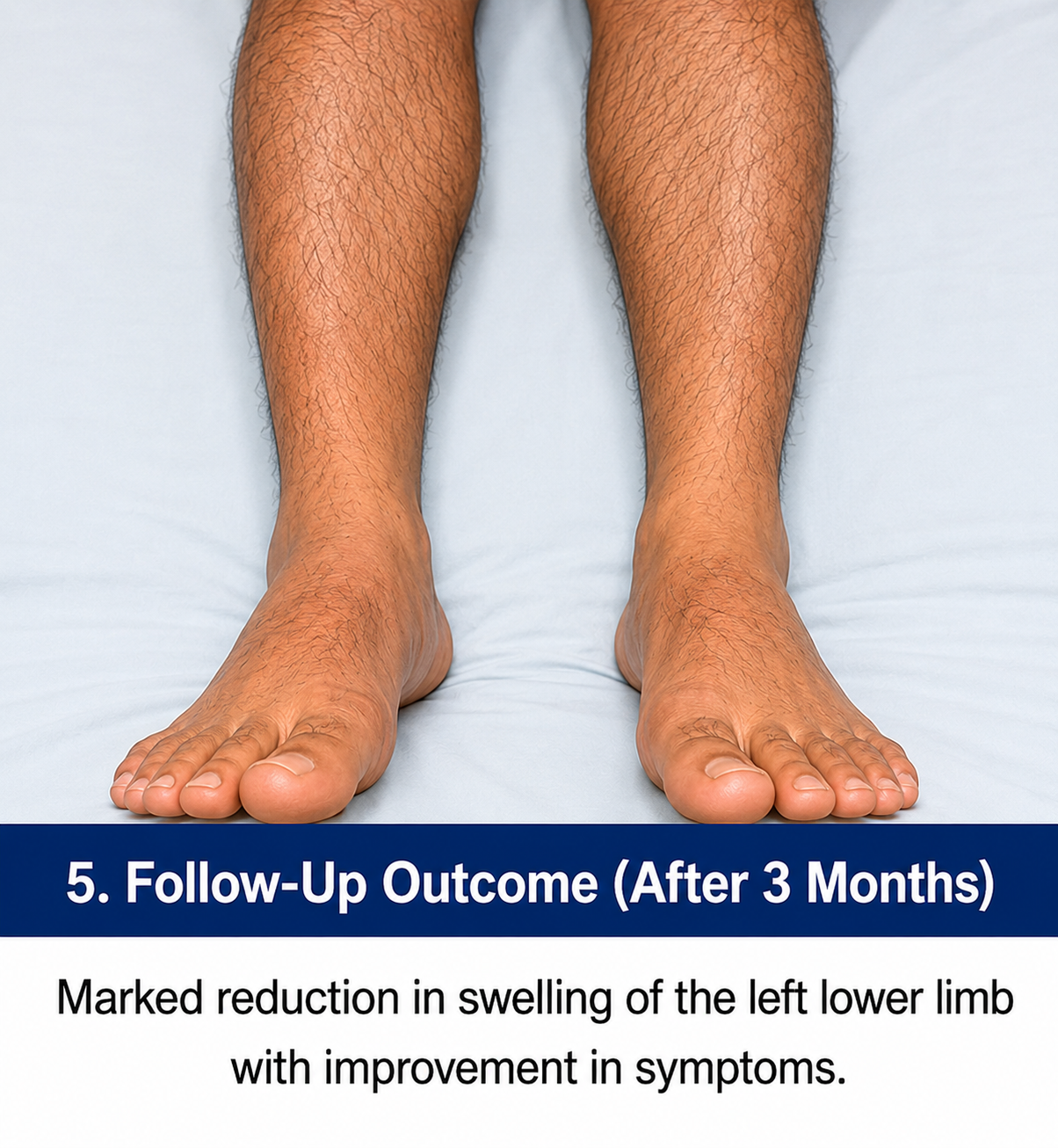
At 3 Months
• Near-complete resolution of edema
• Repeat ultrasonography showed partial recanalization
• No evidence of thrombus extension
At 6 Months
• Complete clinical recovery
• No symptoms of pulmonary embolism
• No recurrence of venous thromboembolism
Anticoagulation was discontinued after six months due to the transient provoking factor.
Discussion
Pathophysiology
Deep vein thrombosis develops through the interaction of factors described in Virchow’s triad.
Venous Stasis
Reduced blood flow occurs during:
• Prolonged immobilization
• Hospitalization
• Paralysis
• Long-distance travel
Endothelial Injury
Damage to the venous endothelium may result from:
• Surgery
• Trauma
• Venous catheterization
Hypercoagulability
Increased clotting tendency may occur due to:
• Malignancy
• Pregnancy
• Hormonal therapy
• Inherited thrombophilia
These mechanisms contribute to thrombus formation within deep veins.
Epidemiology
Important epidemiological features include:
• Annual incidence of approximately 1–2 cases per 1,000 individuals
• Increasing prevalence with advancing age
• Equal occurrence among both genders
• Major contributor to cardiovascular mortality
• Significant healthcare burden worldwide
Venous thromboembolism remains one of the leading preventable causes of hospital-related death.
Clinical Manifestations
Patients with DVT commonly present with:
• Unilateral leg swelling
• Calf pain
• Warmth
• Tenderness
• Erythema
• Limb heaviness
However, some patients may remain asymptomatic.
Severe disease may result in:
• Extensive venous obstruction
• Phlegmasia cerulea dolens
• Pulmonary embolism
• Chronic venous insufficiency
Diagnostic Considerations
Diagnosis is based on:
- Clinical history
- Physical examination
- Wells clinical prediction score
- D-dimer testing
- Compression ultrasonography
- Advanced imaging when required
Compression duplex ultrasonography remains the diagnostic modality of choice for suspected lower-limb DVT.
Treatment Modalities
Anticoagulation Therapy
The cornerstone of DVT management includes:
• Low-molecular-weight heparin
• Direct oral anticoagulants (DOACs)
• Warfarin
Current guidelines favor DOACs in most patients because of efficacy and ease of use.
Mechanical Measures
Supportive interventions include:
• Compression stockings
• Limb elevation
• Early ambulation
Interventional Procedures
Selected patients may require:
• Catheter-directed thrombolysis
• Mechanical thrombectomy
• Inferior vena cava filter placement
These approaches are generally reserved for extensive or high-risk thrombosis.
Complications
Potential complications include:
• Pulmonary embolism
• Recurrent venous thromboembolism
• Post-thrombotic syndrome
• Chronic leg swelling
• Venous ulceration
• Chronic pain
Early diagnosis and treatment substantially reduce these complications.
Prognosis
The prognosis depends on:
• Extent of thrombosis
• Presence of pulmonary embolism
• Timeliness of treatment
• Underlying risk factors
• Patient adherence to therapy
Most patients achieve excellent outcomes with prompt anticoagulation and appropriate follow-up.
Conclusion
Deep vein thrombosis is a potentially serious vascular condition that requires prompt recognition and treatment to prevent life-threatening complications. Careful clinical assessment combined with laboratory evaluation and duplex ultrasonography enables accurate diagnosis. This case demonstrates the successful management of acute proximal deep vein thrombosis following orthopedic surgery through timely anticoagulation therapy, supportive measures, and close follow-up. Early intervention, patient education, and adherence to treatment remain critical for reducing morbidity, preventing recurrence, and improving long-term outcomes.
References
- Kearon C, Akl EA, Ornelas J, et al. Antithrombotic Therapy for VTE Disease. Chest. 2016;149(2):315–352. https://pubmed.ncbi.nlm.nih.gov/26867832/
- Konstantinides SV, Meyer G, Becattini C, et al. ESC Guidelines for Acute Pulmonary Embolism. Eur Heart J. 2020;41(4):543–603. https://pubmed.ncbi.nlm.nih.gov/31504429/
- Ortel TL, Neumann I, Ageno W, et al. American Society of Hematology Guidelines for VTE Management. Blood Adv. 2020;4(19):4693–4738. https://pmc.ncbi.nlm.nih.gov/articles/PMC7556153/
- Di Nisio M, van Es N, Buller HR. Deep Vein Thrombosis and Pulmonary Embolism. Lancet. 2016;388(10063):3060–3073. https://pubmed.ncbi.nlm.nih.gov/27375038/
- Heit JA. Epidemiology of Venous Thromboembolism. Nat Rev Cardiol. 2015;12(8):464–474. https://pubmed.ncbi.nlm.nih.gov/26076949/
- Tritschler T, Kraaijpoel N, Le Gal G, Wells PS. Venous Thromboembolism: Advances in Diagnosis and Treatment. JAMA. 2018;320(15):1583–1594. https://pubmed.ncbi.nlm.nih.gov/30398601/
- Kahn SR, Comerota AJ, Cushman M, et al. Post-Thrombotic Syndrome. J Thromb Haemost. 2014;12(6):879–885. https://pubmed.ncbi.nlm.nih.gov/24750768/
- Huisman MV, Barco S, Cannegieter SC, et al. Pulmonary Embolism. Nat Rev Dis Primers. 2018;4:18028. https://pubmed.ncbi.nlm.nih.gov/29884811/
- Weitz JI, Bauersachs R, Beyer-Westendorf J, et al. Anticoagulation for VTE. Circulation. 2020;142(17):1599–1613. https://pubmed.ncbi.nlm.nih.gov/33059498/
- Raskob GE, Angchaisuksiri P, Blanco AN, et al. Thrombosis: A Major Contributor to Global Disease Burden. Arterioscler Thromb Vasc Biol. 2014;34(11):2363–2371. https://pubmed.ncbi.nlm.nih.gov/25304324/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge