Onychomycosis: Clinical Presentation, Diagnostic Evaluation, Antifungal Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Onychomycosis is a common fungal infection of the nails caused primarily by dermatophytes, yeasts, and non-dermatophyte molds. It accounts for approximately 50% of all nail disorders and significantly affects quality of life due to cosmetic concerns, discomfort, and functional impairment. The condition commonly presents with nail discoloration, thickening, brittleness, subungual debris, and progressive nail destruction.
Accurate diagnosis requires careful clinical examination supported by laboratory confirmation through microscopy, fungal culture, or molecular techniques. Early diagnosis and appropriate antifungal therapy are essential to prevent disease progression and recurrence.
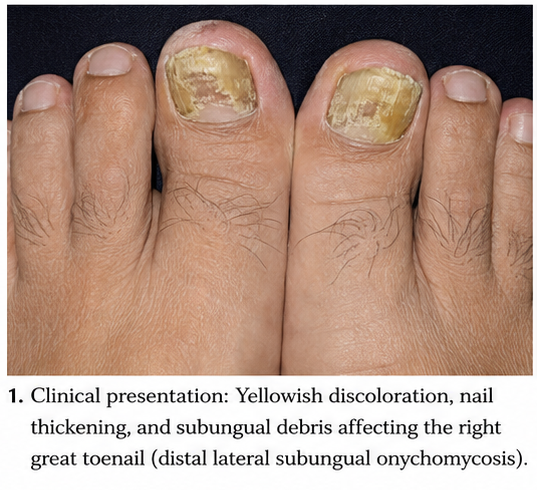
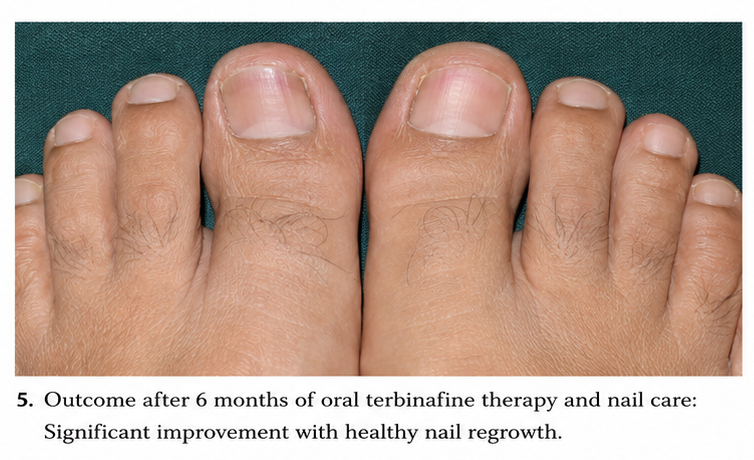
We present the case of a 52-year-old male who presented with progressive discoloration and thickening of the toenails associated with difficulty trimming the nails and discomfort while walking. Clinical examination, potassium hydroxide (KOH) microscopy, and fungal culture confirmed distal lateral subungual onychomycosis caused by Trichophyton rubrum. The patient was successfully treated with oral terbinafine and supportive nail care, resulting in significant clinical improvement and healthy nail regrowth.
This case highlights the importance of early recognition, laboratory confirmation, and comprehensive treatment strategies in achieving favorable outcomes in patients with onychomycosis.
Introduction
Onychomycosis refers to a fungal infection affecting the nail unit, including the nail plate, nail bed, and surrounding tissues. It is one of the most common nail disorders encountered in dermatological practice and represents a substantial healthcare burden worldwide.
The condition is predominantly caused by dermatophytes, particularly Trichophyton rubrum and Trichophyton interdigitale, although yeasts such as Candida species and non-dermatophyte molds may also be responsible.
Common risk factors for onychomycosis include:
• Advanced age
• Diabetes mellitus
• Peripheral vascular disease
• Immunosuppression
• Repeated nail trauma
• Hyperhidrosis
• Tinea pedis
• Use of occlusive footwear
The infection may lead to progressive nail dystrophy, discomfort, secondary bacterial infections, and psychosocial distress. Prompt diagnosis and treatment are therefore essential.
Case Report
Patient History
A 52-year-old male presented to the dermatology outpatient department with complaints of:
• Progressive yellow discoloration of the right great toenail for 12 months
• Thickening of the affected nail
• Difficulty trimming the nail
• Mild discomfort while walking
• Cosmetic concerns regarding nail appearance
The patient reported gradual progression of symptoms over the preceding year. There was no history of acute trauma or significant pain.
Additional history revealed:
• Long-standing tinea pedis for several years
• Excessive sweating of the feet
• Frequent use of closed footwear during work
Past medical history included:
• Type 2 diabetes mellitus for 8 years
• Hypertension controlled with medication
There was no history of:
• Psoriasis
• Recent nail surgery
• Immunosuppressive therapy
• Peripheral neuropathy
Clinical Examination
General Examination
• Blood pressure: 130/82 mmHg
• Pulse rate: 78/min
• Temperature: Afebrile
• General condition: Stable
Dermatological Examination
Inspection revealed:
• Yellow-brown discoloration of the right great toenail
• Marked nail plate thickening
• Subungual hyperkeratosis
• Distal nail separation from the nail bed (onycholysis)
The nail surface appeared rough and brittle.
Associated findings included:
• Interdigital scaling between the toes
• Mild plantar erythema consistent with tinea pedis
No evidence of surrounding cellulitis or secondary bacterial infection was observed.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Onychomycosis
• Nail psoriasis
• Traumatic nail dystrophy
• Lichen planus involving nails
• Chronic paronychia
The presence of subungual hyperkeratosis, nail discoloration, and concurrent tinea pedis strongly suggested fungal nail infection.
Investigations
Laboratory Evaluation
Routine investigations demonstrated:
• Hemoglobin: 13.6 g/dL
• Total leukocyte count: 7,800/mm³
• Blood glucose: Mildly elevated
• Renal function tests: Normal
• Liver function tests: Normal
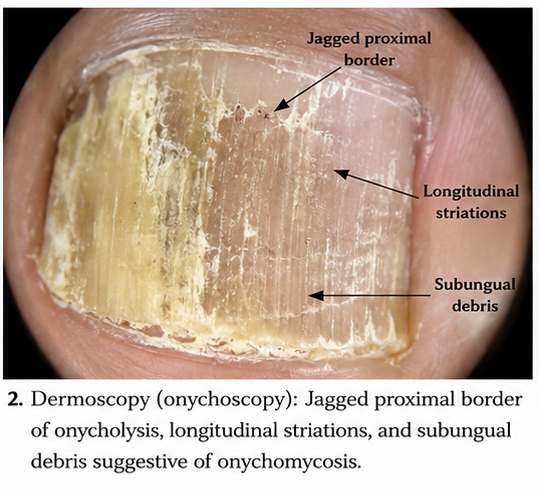
Dermoscopy
Onychoscopy demonstrated:
• Jagged proximal border of onycholysis
• Longitudinal streaks
• Subungual debris
These findings further supported the diagnosis of onychomycosis.
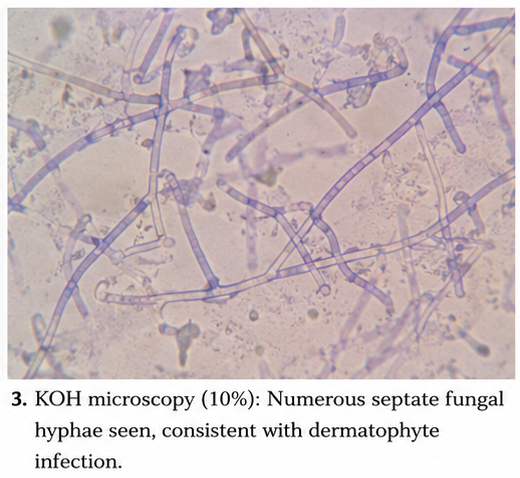
Potassium Hydroxide (KOH) Microscopy
Nail scrapings were obtained from the affected area.
Microscopic examination demonstrated:
• Septate fungal hyphae
• Positive findings consistent with dermatophyte infection
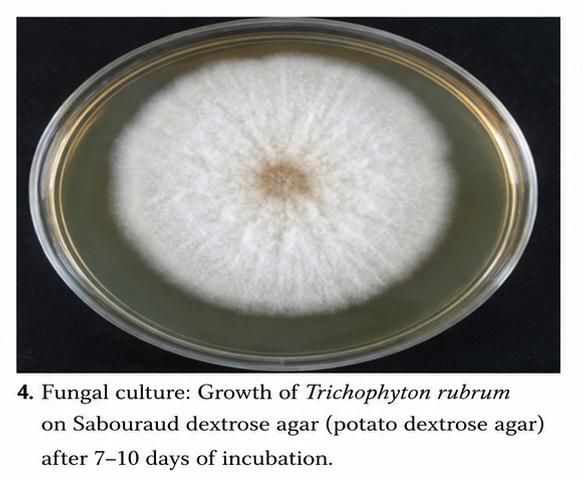
Fungal Culture
Culture of nail samples revealed:
• Growth of Trichophyton rubrum
Diagnosis
Based on clinical examination, microscopy, and fungal culture, a diagnosis of:
Distal Lateral Subungual Onychomycosis Caused by Trichophyton rubrum
was established.
Management and Outcome
Initial Management
The patient was counseled regarding the chronic nature of the disease and the importance of treatment adherence.
Treatment included:
• Oral terbinafine 250 mg once daily
• Mechanical nail trimming and debridement
• Treatment of concurrent tinea pedis
• Advice regarding foot hygiene
Additional recommendations included:
• Keeping feet dry
• Regular sock changes
• Avoidance of sharing footwear
• Use of antifungal powders
Follow-Up and Clinical Course
At 6 Weeks
• Reduced nail discoloration progression
• Improvement in surrounding skin lesions
• Good treatment adherence
At 3 Months
• Significant reduction in subungual debris
• Healthier proximal nail growth observed
• No adverse drug reactions
At 6 Months
• Marked improvement in nail appearance
• Resolution of discomfort during walking
• Nearly complete replacement of diseased nail
At 9 Months
• Complete clinical recovery
• Healthy nail plate regrowth
• No evidence of recurrence
Discussion
Pathophysiology
Onychomycosis develops when fungal organisms invade the nail unit and establish persistent infection. Dermatophytes possess keratinolytic enzymes that facilitate penetration and colonization of keratinized structures.
Several factors contribute to disease development:
• Warm and moist environments
• Repeated microtrauma
• Reduced peripheral circulation
• Impaired immune function
• Presence of tinea pedis
The infection commonly begins at the distal nail edge and gradually progresses proximally.
Epidemiology
Important epidemiological features include:
• Onychomycosis affects approximately 5–15% of the global population
• Prevalence increases with age
• Men are affected more frequently than women
• Diabetes significantly increases susceptibility
• Toenails are affected more commonly than fingernails
Dermatophytes remain the leading causative organisms worldwide.
Clinical Manifestations
Patients with onychomycosis commonly present with:
• Nail discoloration
• Thickened nails
• Brittle nail texture
• Subungual debris
• Nail plate distortion
• Difficulty cutting nails
Advanced disease may result in:
• Pain during walking
• Secondary bacterial infection
• Functional impairment
• Psychosocial distress
Diagnostic Considerations
Diagnosis is based on:
- Clinical history
- Physical examination
- KOH microscopy
- Fungal culture
- Histopathological examination when necessary
- Molecular diagnostic techniques in selected cases
Laboratory confirmation is important because several nail disorders can mimic fungal infection.
Treatment Modalities
Topical Therapy
Suitable for mild disease:
• Ciclopirox nail lacquer
• Efinaconazole solution
• Tavaborole solution
Systemic Therapy
Oral antifungal agents remain the gold standard for extensive disease.
Common medications include:
• Terbinafine
• Itraconazole
• Fluconazole
Terbinafine is generally preferred due to high cure rates and favorable safety profile.
Adjunctive Measures
Supportive management includes:
• Nail debridement
• Foot hygiene optimization
• Treatment of tinea pedis
• Preventive education
Complications
Potential complications include:
• Permanent nail dystrophy
• Secondary bacterial infection
• Pain and mobility limitation
• Recurrent infection
• Spread to adjacent nails
Early treatment significantly reduces these complications.
Prognosis
The prognosis depends on:
• Extent of nail involvement
• Causative organism
• Presence of comorbidities
• Treatment adherence
• Duration of infection
Patients receiving appropriate antifungal therapy generally experience excellent outcomes, although recurrence remains possible.
Conclusion
Onychomycosis is a common fungal nail infection that can significantly impact physical comfort, nail function, and quality of life. Careful clinical assessment combined with laboratory confirmation is essential for establishing an accurate diagnosis and guiding appropriate therapy. This case demonstrates the successful management of distal lateral subungual onychomycosis caused by Trichophyton rubrum through oral antifungal treatment, nail care, and preventive measures. Early diagnosis, patient education, and adherence to therapy remain critical for achieving favorable outcomes and minimizing recurrence.
References
- Lipner SR, Scher RK. Onychomycosis: Clinical overview and diagnosis. J Am Acad Dermatol. 2019;80(4):835–851. https://pubmed.ncbi.nlm.nih.gov/30691753/
- Gupta AK, Versteeg SG. Onychomycosis therapy: Past, present, future. J Fungi. 2017;3(4):56. https://pmc.ncbi.nlm.nih.gov/articles/PMC5770011/
- Piraccini BM, Alessandrini A. Onychomycosis: A review. J Fungi. 2015;1(1):30–43. https://pmc.ncbi.nlm.nih.gov/articles/PMC5770012/
- Westerberg DP, Voyack MJ. Onychomycosis: Current trends in diagnosis and treatment. Am Fam Physician. 2013;88(11):762–770. https://pubmed.ncbi.nlm.nih.gov/24364524/
- Gupta AK, Mays RR. The impact of onychomycosis on quality of life. Skin Appendage Disord. 2018;4(4):208–216. https://pmc.ncbi.nlm.nih.gov/articles/PMC6249733/
- Scher RK, Tavakkol A, Sigurgeirsson B, et al. Onychomycosis: Diagnosis and definition of cure. J Am Acad Dermatol. 2007;56(6):939–944. https://pubmed.ncbi.nlm.nih.gov/17504709/
- Elewski BE, Rich P, Pollak R, et al. Efinaconazole topical solution for onychomycosis. J Drugs Dermatol. 2013;12(2):186–192. https://pubmed.ncbi.nlm.nih.gov/23377374/
- Ameen M, Lear JT, Madan V, et al. British Association of Dermatologists’ guidelines for management of onychomycosis. Br J Dermatol. 2014;171(5):937–958. https://pubmed.ncbi.nlm.nih.gov/25209742/
- Leung AKC, Lam JM, Leong KF, et al. Onychomycosis: An updated review. Recent Pat Inflamm Allergy Drug Discov. 2020;14(1):32–45. https://pubmed.ncbi.nlm.nih.gov/31663326/
- Gupta AK, Foley KA. Evidence-based management of onychomycosis. Am J Clin Dermatol. 2019;20(6):839–851. https://pubmed.ncbi.nlm.nih.gov/31468220/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge