Vulvovaginal Candidiasis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
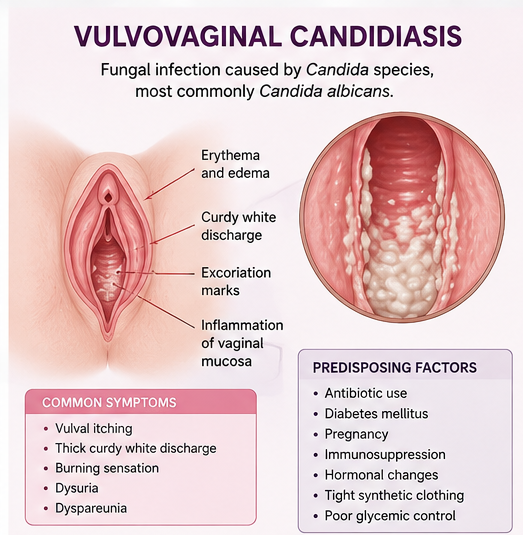
Vulvovaginal candidiasis (VVC) is one of the most common fungal infections affecting women of reproductive age. It is primarily caused by Candida albicans and presents with vulval itching, curdy vaginal discharge, burning sensation, dyspareunia, and dysuria. Although uncomplicated infections respond well to antifungal therapy, recurrent or severe disease may significantly impair quality of life and require prolonged management.
We present the case of a 32-year-old female who presented with intense vulval itching, thick white vaginal discharge, dysuria, and discomfort during intercourse for 10 days. Clinical examination, vaginal pH assessment, microscopy, and fungal culture confirmed vulvovaginal candidiasis caused by Candida albicans. The patient was treated with oral fluconazole, topical antifungal therapy, lifestyle modifications, and counseling regarding recurrence prevention, resulting in significant symptomatic improvement.
This case highlights the importance of early diagnosis, identification of predisposing factors, appropriate antifungal therapy, and patient education in the effective management of vulvovaginal candidiasis.
Introduction
Vulvovaginal candidiasis is a common fungal infection involving the vulva and vaginal mucosa, predominantly caused by Candida albicans. It affects nearly 75% of women at least once during their lifetime, while recurrent vulvovaginal candidiasis occurs in approximately 5–8% of women.
The disease occurs when alterations in the vaginal microenvironment allow overgrowth of Candida species. Factors such as antibiotic use, uncontrolled diabetes mellitus, pregnancy, immunosuppression, hormonal changes, and poor genital hygiene contribute to increased susceptibility.
Several mechanisms contribute to disease development, including:
- Alteration of normal vaginal flora
- Increased vaginal glycogen content
- Hormonal influences
- Local immune dysfunction
- Enhanced fungal adhesion to epithelial cells
Important risk factors include:
- Recent antibiotic therapy
- Diabetes mellitus
- Pregnancy
- Immunosuppression
- Oral contraceptive use
- Tight synthetic clothing
- Poor glycemic control
- Recurrent moisture exposure
Common symptoms include:
- Vulval itching
- Thick curdy white vaginal discharge
- Burning sensation
- Dysuria
- Dyspareunia
- Vulval erythema and edema
- Vaginal soreness
Early diagnosis and targeted therapy are essential to prevent recurrent infections and improve patient comfort and quality of life.
Case Report
Patient History
A 32-year-old married female presented to the gynecology outpatient department with:
- Severe vulval itching for 10 days
- Thick white vaginal discharge
- Burning sensation during urination
- Vaginal soreness
- Pain during sexual intercourse
The patient reported progressive worsening of symptoms over the previous week, causing discomfort during daily activities and sleep disturbance.
History revealed recent antibiotic use for upper respiratory tract infection two weeks earlier.
There was no history of:
- Sexually transmitted infections
- Pelvic inflammatory disease
- Tuberculosis
- Recent gynecological procedures
- Malignancy
The patient had a known history of type 2 diabetes mellitus with irregular glycemic control.
Clinical Examination
General Examination
- Afebrile
- Pulse rate: 82/min
- Blood pressure: 118/76 mmHg
- Body mass index: 25 kg/m²
- Systemically stable
Gynecological Examination
Local examination revealed:
- Vulval erythema
- Edema of labia
- Excoriation marks due to scratching
- Thick curdy white vaginal discharge adherent to vaginal walls
- Vaginal mucosal inflammation
No cervical erosion or pelvic tenderness was noted.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
- Bacterial vaginosis
- Trichomoniasis
- Allergic vulvovaginitis
- Sexually transmitted infections
- Vulvovaginal candidiasis
The presence of intense pruritus, curdy white discharge, erythema, and recent antibiotic exposure strongly suggested vulvovaginal candidiasis.
Investigations
Laboratory Findings
- Random blood glucose: Elevated
- HbA1c: Poor glycemic control
- Complete blood count: Mild leukocytosis
- Urine routine examination: No urinary tract infection
Vaginal pH Testing
- Vaginal pH: 4.2
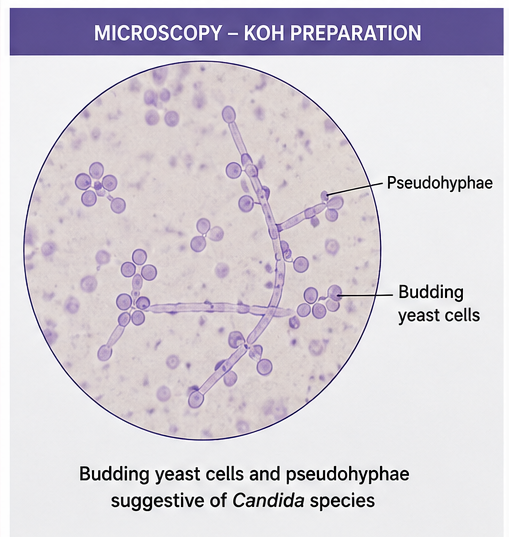
Microscopy
Wet mount and potassium hydroxide (KOH) preparation demonstrated:
- Budding yeast cells
- Pseudohyphae
- Fungal elements suggestive of Candida species
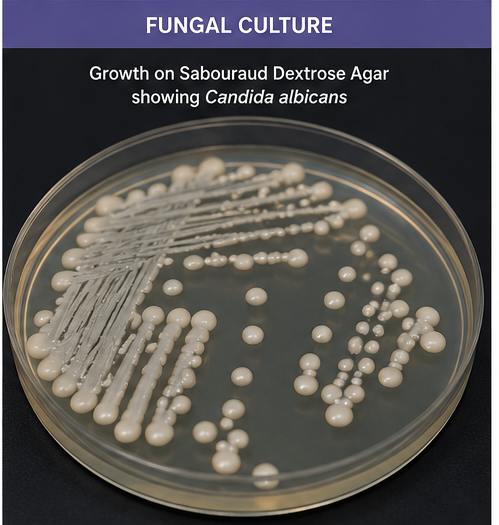
Fungal Culture
Culture on Sabouraud dextrose agar showed growth of Candida albicans.
Diagnosis
Based on clinical presentation, vaginal examination, microscopy findings, and fungal culture, a diagnosis of Acute Vulvovaginal Candidiasis caused by Candida albicans was established.
Management and Outcome
Initial Management
The patient was counseled regarding:
- Nature of fungal infection
- Importance of genital hygiene
- Glycemic control
- Avoidance of self-medication
- Risk of recurrence
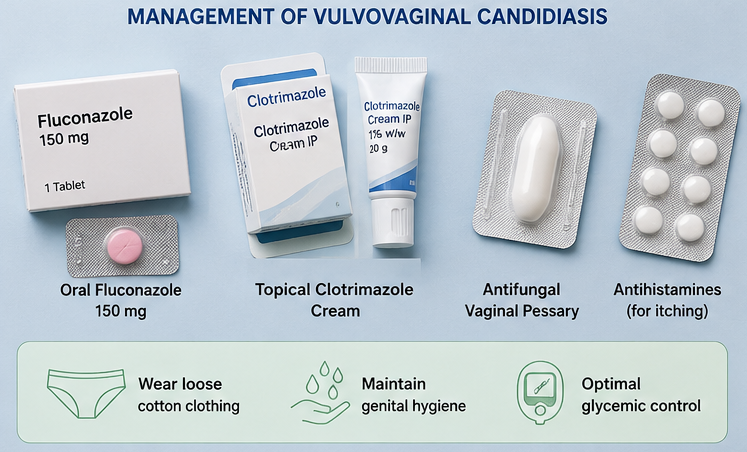
Medical Management
The patient received:
- Oral fluconazole 150 mg single dose
- Topical clotrimazole cream
- Antifungal vaginal pessary
- Antihistamines for itching
- Advice regarding loose cotton clothing
- Diabetic management optimization
Follow-Up and Clinical Course
At 1 Week
- Significant reduction in itching
- Reduced vaginal discharge
- Improvement in burning sensation
At 2 Weeks
- Complete symptomatic relief
- Resolution of vulval erythema
- Improved sleep and comfort
At 1 Month
- No recurrence of symptoms
- Better glycemic control achieved
- Patient educated regarding preventive measures
The patient remained under periodic gynecological and diabetic follow-up.
Discussion
Pathophysiology
Vulvovaginal candidiasis results from overgrowth of Candida species within the vaginal mucosa following disruption of the normal vaginal ecosystem.
Important pathological mechanisms include:
- Overgrowth of Candida organisms
- Adhesion to vaginal epithelial cells
- Biofilm formation
- Local inflammatory response
- Alteration in vaginal flora
Hyperglycemia enhances fungal proliferation and increases susceptibility to recurrent infection.
Epidemiology
Important epidemiological features include:
- Affects nearly 75% of women at least once
- Most common during reproductive years
- Increased incidence during pregnancy
- Frequently associated with diabetes mellitus
- Recurrent disease affects approximately 5–8% of women
Clinical Manifestations
Common manifestations include:
-
Vulval itching
- Curdy white discharge
- Vaginal soreness
- Burning sensation
- Dyspareunia
- Dysuria
- Vulval swelling
Signs commonly observed include:
- Erythema
- Vaginal inflammation
- Excoriations
- Edema
- Thick adherent discharge
Diagnostic Considerations
Diagnosis is primarily clinical but supported by laboratory evaluation.
Important diagnostic modalities include:
- Vaginal pH assessment
- Wet mount microscopy
- KOH preparation
- Fungal culture
- Molecular diagnostic tests
Microscopy demonstrating budding yeast cells and pseudohyphae strongly supports diagnosis.
Treatment Modalities
Conservative Measures
Supportive recommendations include:
- Maintaining genital hygiene
- Avoiding tight clothing
- Controlling diabetes
- Avoiding unnecessary antibiotics
- Using breathable cotton undergarments
Pharmacological Therapy
Common antifungal treatments include:
- Fluconazole
- Clotrimazole
- Miconazole
- Nystatin
- Topical azoles
Recurrent infections may require prolonged suppressive antifungal therapy.
Complications
Potential complications include:
- Recurrent vulvovaginal candidiasis
- Severe vulval excoriation
- Secondary bacterial infection
- Sexual dysfunction
- Psychological distress
- Reduced quality of life
Untreated recurrent infections may lead to chronic vulvovaginal discomfort.
Prognosis
The prognosis depends upon:
- Early diagnosis
- Adequate antifungal therapy
- Glycemic control
- Prevention of recurrence
- Patient adherence to treatment
Most uncomplicated cases respond well to standard antifungal therapy.
Conclusion
Vulvovaginal candidiasis is a common fungal infection that can significantly affect comfort, sexual health, and quality of life among women of reproductive age. Early recognition of vulval itching, curdy vaginal discharge, and vaginal irritation is essential for timely diagnosis and treatment.
This case highlights the importance of clinical evaluation, laboratory confirmation, antifungal therapy, glycemic optimization, and patient education in achieving favorable clinical outcomes. Prevention of recurrence through lifestyle modification and management of underlying risk factors remains an essential component of comprehensive care.
References
- Sobel JD. Vulvovaginal candidosis. https://pubmed.ncbi.nlm.nih.gov/15315592/
- Willems HME, Ahmed SS, Liu J, Xu Z, Peters BM. Vulvovaginal candidiasis: A current understanding and burning questions. https://pubmed.ncbi.nlm.nih.gov/30256738/
- Centers for Disease Control and Prevention. Vulvovaginal Candidiasis Guidelines. https://www.cdc.gov/std/treatment-guidelines/candidiasis.htm
- Pappas PG, Kauffman CA, Andes DR, et al. Clinical Practice Guideline for the Management of Candidiasis. https://pubmed.ncbi.nlm.nih.gov/26679628/
- Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines. https://pubmed.ncbi.nlm.nih.gov/34292926/
- World Health Organization. Sexual and reproductive health guidelines. https://www.who.int/health-topics/sexual-health
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge