Pressure Ulcer (Bedsore) in a Bedridden Elderly Patient: A Case Report
OthersPage Navigation
Abstract
Pressure ulcers, commonly known as bedsores or pressure injuries, are localized injuries to the skin and underlying tissues caused by prolonged pressure, shear, or friction over bony prominences. They are a major source of morbidity among elderly, immobilized, and critically ill patients, often leading to prolonged hospitalization, secondary infections, and reduced quality of life. Early identification of at-risk patients, comprehensive wound assessment, pressure redistribution, infection control, nutritional optimization, and appropriate wound care are essential for successful healing. We report the case of a 72-year-old bedridden man with a Stage III sacral pressure ulcer that developed following prolonged immobilization after an ischemic stroke. The patient underwent surgical debridement, culture-guided antibiotic therapy, advanced wound dressings, nutritional supplementation, and pressure-relieving interventions. Over six months of multidisciplinary management, significant wound healing with complete granulation tissue formation and restoration of skin integrity was achieved. This case highlights the importance of early intervention and multidisciplinary care in the successful management of pressure ulcers.
Introduction
Pressure ulcers are among the most common preventable complications affecting bedridden and immobilized patients. They occur when prolonged pressure exceeds capillary perfusion pressure, leading to tissue ischemia, hypoxia, and eventual necrosis. The sacrum, heels, greater trochanters, ischial tuberosities, and elbows are the most frequently affected anatomical sites due to sustained pressure over bony prominences.
The incidence of pressure ulcers remains high among elderly individuals, particularly those with neurological disorders, spinal cord injuries, prolonged intensive care admissions, diabetes mellitus, malnutrition, and reduced mobility. Besides causing pain and impaired quality of life, pressure ulcers significantly increase healthcare costs and are associated with serious complications including cellulitis, osteomyelitis, sepsis, and mortality.
Management requires a multidisciplinary approach involving pressure offloading, wound bed preparation, infection control, adequate nutrition, glycemic optimization, and patient as well as caregiver education. Early recognition and timely treatment remain the cornerstones of preventing disease progression and improving clinical outcomes.
Case Report
A 72-year-old man presented to the wound care clinic with a painful ulcer over the sacral region that had progressively worsened over the previous three weeks. The patient had suffered an ischemic stroke five months earlier, resulting in left-sided hemiplegia and prolonged confinement to bed. His medical history included poorly controlled type 2 diabetes mellitus and hypertension. According to his caregiver, prolonged sitting and lying in one position, reduced nutritional intake, and urinary incontinence contributed to the development of the wound.
On examination, the patient appeared mildly cachectic but was hemodynamically stable. Local examination revealed a 7 × 6 cm ulcer over the sacrum with full-thickness skin loss extending into the subcutaneous tissue. The wound contained areas of slough and moderate seropurulent discharge with surrounding erythema. There was localized tenderness without evidence of exposed bone or deep sinus formation. Based on the National Pressure Injury Advisory Panel (NPIAP) classification, the lesion was diagnosed as a Stage III pressure ulcer.
Laboratory investigations demonstrated leukocytosis (13,200 cells/mm³), elevated C-reactive protein (48 mg/L), erythrocyte sedimentation rate of 52 mm/hour, fasting blood glucose of 196 mg/dL, and HbA1c of 8.5%. Serum albumin was reduced at 2.9 g/dL, indicating poor nutritional status. Wound culture isolated methicillin-sensitive Staphylococcus aureus (MSSA), while blood cultures remained sterile. Pelvic radiography showed no evidence of underlying osteomyelitis.
Based on the clinical findings and investigations, a diagnosis of Stage III infected sacral pressure ulcer associated with prolonged immobilization was established.
Management and Outcome
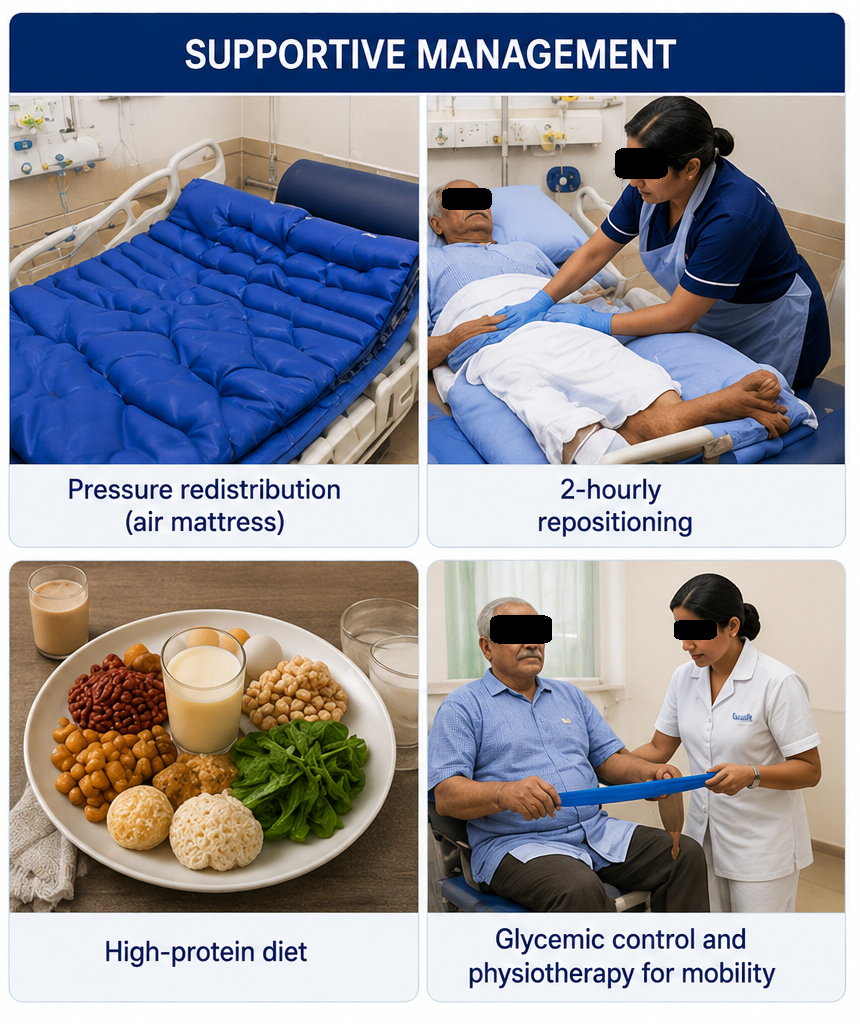
The patient was admitted for comprehensive multidisciplinary management. Pressure redistribution was achieved using a dynamic air mattress, and caregivers were instructed to reposition the patient every two hours. Surgical debridement was performed to remove necrotic tissue and establish a healthy wound bed.
Intravenous antibiotics were initiated according to culture sensitivity results and continued for ten days before transitioning to oral therapy. Advanced moist wound dressings containing hydrofiber and antimicrobial agents were applied with regular dressing changes under sterile conditions.
A clinical nutritionist prescribed a high-protein diet enriched with arginine, zinc, vitamin C, and multivitamin supplementation to facilitate wound healing. Blood glucose levels were optimized using insulin therapy under endocrinology supervision. Physiotherapy was initiated to improve mobility, reduce pressure duration, and prevent further complications.
No complications such as osteomyelitis, systemic infection, or wound deterioration occurred during hospitalization.
Follow-up
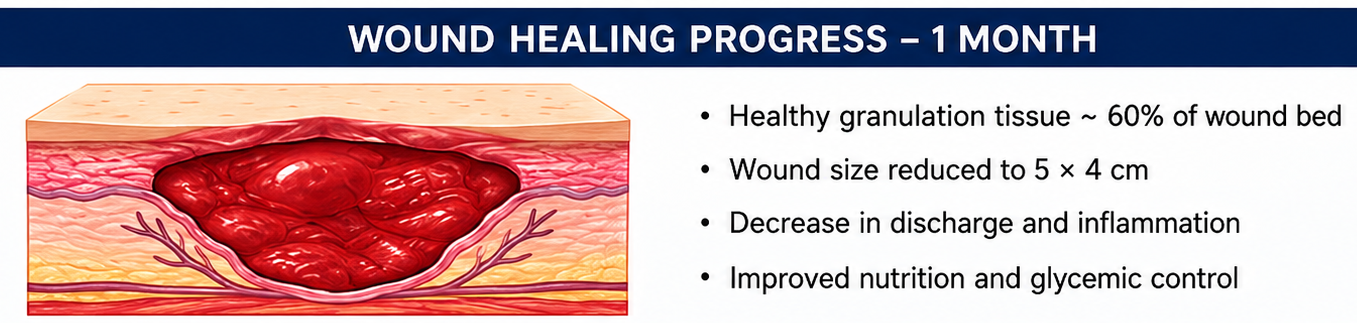
One Month
- Healthy granulation tissue covered approximately 60% of the wound bed.
- Reduction in wound size to 5 × 4 cm.
- Significant decrease in wound discharge and surrounding inflammation.
- Improved nutritional status and glycemic control.
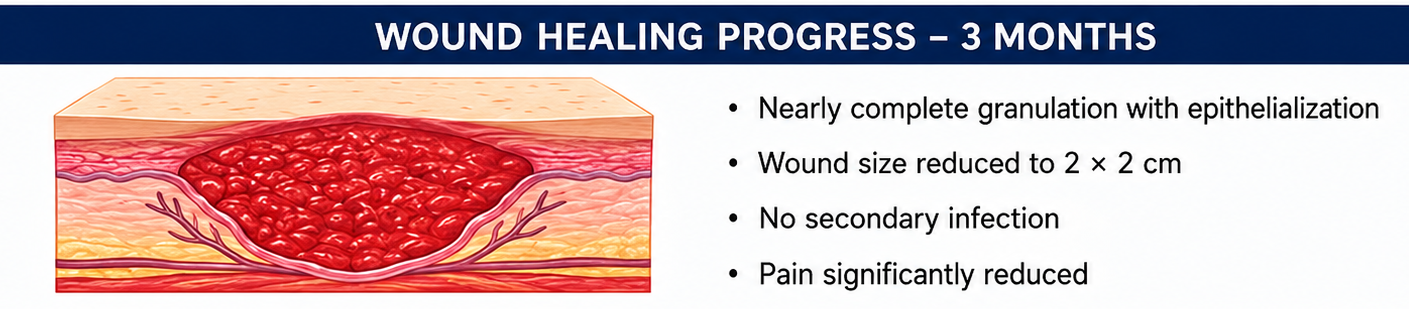
Three Months
- Nearly complete granulation with progressive epithelialization.
- Wound dimensions reduced to 2 × 2 cm.
- No evidence of secondary infection.
- Patient tolerated sitting for short periods using pressure-relieving cushions.
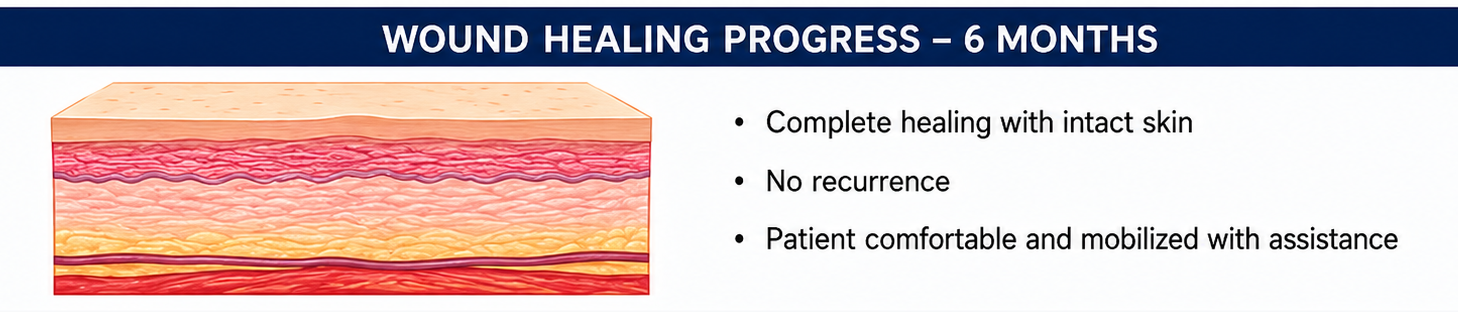
Six Months
Complete wound healing was achieved with healthy scar formation. The patient remained free of recurrence during follow-up. Caregivers continued pressure-relieving measures, nutritional support, and regular skin inspections to prevent future pressure injuries.
Discussion
Pressure ulcers remain an important healthcare challenge worldwide despite being largely preventable. Tissue damage develops when prolonged pressure compromises capillary blood flow, leading to ischemia, inflammation, and necrosis. Shear forces, friction, excessive moisture, malnutrition, advanced age, neurological impairment, diabetes mellitus, and vascular disease further increase susceptibility.
The sacrum is the most common site for pressure ulcer development in bedridden patients because it bears continuous pressure in the supine position. Accurate staging using the NPIAP classification guides treatment decisions and prognosis.
Successful management requires comprehensive wound assessment, removal of necrotic tissue, control of bacterial burden, maintenance of an optimal moist wound environment, nutritional optimization, and effective pressure redistribution. Surgical debridement remains the gold standard for removing devitalized tissue in Stage III and Stage IV pressure ulcers.
Adequate nutritional support is equally important because protein-energy malnutrition delays collagen synthesis, angiogenesis, and immune function. Supplementation with protein, arginine, zinc, and vitamins has been shown to improve healing rates in patients with chronic wounds.
Pressure redistribution using specialized mattresses, frequent repositioning, heel protection devices, and caregiver education significantly reduces tissue loading and recurrence. Infection should always be suspected in wounds with increasing pain, purulent discharge, foul odor, delayed healing, or surrounding cellulitis. Culture-guided antibiotic therapy should be reserved for clinically infected wounds rather than simple colonization.
Early multidisciplinary intervention involving wound care specialists, surgeons, physicians, dietitians, physiotherapists, and nursing staff offers the highest likelihood of complete healing while minimizing complications such as osteomyelitis, sepsis, prolonged hospitalization, and recurrent ulceration.
Prognosis
The prognosis of pressure ulcers depends on ulcer stage, nutritional status, comorbid illnesses, infection control, and adherence to pressure-relieving strategies. Stage III pressure ulcers generally respond well to comprehensive multidisciplinary management when diagnosed early. Delayed treatment may result in chronic non-healing wounds, osteomyelitis, septicemia, prolonged hospitalization, and increased mortality. Continuous preventive care remains essential even after complete healing because recurrence rates remain high among chronically immobilized patients.
Conclusion
Pressure ulcers remain a significant but largely preventable complication among bedridden patients. Early risk assessment, prompt diagnosis, pressure redistribution, surgical debridement when indicated, infection control, nutritional optimization, and comprehensive multidisciplinary care are fundamental to successful treatment. This case demonstrates that timely intervention combined with caregiver education and long-term preventive strategies can achieve complete wound healing and substantially improve patient outcomes.
References
- European Pressure Ulcer Advisory Panel (EPUAP), National Pressure Injury Advisory Panel (NPIAP), and Pan Pacific Pressure Injury Alliance (PPPIA). Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. https://www.internationalguideline.com/
- Jaul E, Barron J. Age-related diseases and clinical and public health implications for the 85 years old and over population. Front Public Health. 2017;5:335. https://pubmed.ncbi.nlm.nih.gov/29312964/
- Padula WV, Delarmente BA. The National Pressure Injury Advisory Panel pressure injury stages: Updated staging system. Adv Skin Wound Care. 2019;32(6):269–275. https://pubmed.ncbi.nlm.nih.gov/31095011/
- Li Z, Lin F, Thalib L, Chaboyer W. Global prevalence and incidence of pressure injuries in hospitalised adult patients: A systematic review and meta-analysis. Int J Nurs Stud. 2020;105:103546. https://pubmed.ncbi.nlm.nih.gov/32028126/
- Gaspar S, Peralta M, Marques A, Budri A, Ferreira F. Effectiveness on hospital-acquired pressure ulcer prevention: A systematic review. Int Wound J. 2019;16(5):1087–1102. https://pubmed.ncbi.nlm.nih.gov/31190368/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge