Retinal Edema Secondary to Branch Retinal Vein Occlusion: A Case Report
OthersPage Navigation
Abstract
Retinal edema is one of the leading causes of visual impairment associated with retinal vascular disorders, particularly branch retinal vein occlusion (BRVO). The condition results from increased vascular permeability secondary to retinal ischemia and vascular endothelial growth factor (VEGF) overexpression, leading to accumulation of intraretinal fluid within the macula. Early diagnosis using optical coherence tomography (OCT) and prompt treatment with intravitreal anti-VEGF agents have significantly improved visual outcomes. We report the case of a 62-year-old woman who presented with sudden painless blurring of vision in her left eye for one week. Fundus examination demonstrated retinal hemorrhages with macular edema involving the superotemporal quadrant. OCT confirmed cystoid retinal edema with increased central macular thickness, while fluorescein angiography revealed delayed venous filling consistent with branch retinal vein occlusion. The patient received three monthly intravitreal aflibercept injections, resulting in marked reduction of retinal edema and significant improvement in visual acuity. This case emphasizes the importance of early recognition and timely intervention in retinal edema secondary to retinal vein occlusion to preserve visual function.
Introduction
Retinal edema refers to the abnormal accumulation of extracellular or intracellular fluid within the retinal layers, most commonly involving the macula. It develops secondary to disruption of the inner or outer blood-retinal barrier, resulting in increased vascular permeability and fluid leakage. Retinal edema is commonly associated with diabetic retinopathy, retinal vein occlusion, uveitis, postoperative inflammation, and retinal vascular diseases.
Branch retinal vein occlusion is the second most common retinal vascular disorder after diabetic retinopathy. Venous obstruction causes increased capillary hydrostatic pressure, retinal ischemia, and release of VEGF and inflammatory cytokines, leading to macular edema - the primary cause of visual loss in affected patients. Advances in retinal imaging, particularly spectral-domain OCT, have revolutionized diagnosis and monitoring, while intravitreal anti-VEGF therapy has become the standard first-line treatment. Early intervention is associated with superior anatomical and functional recovery.
Case Report
A 62-year-old woman presented to the ophthalmology outpatient department with sudden painless diminution of vision in her left eye for seven days. She described blurred central vision and difficulty reading but denied flashes, floaters, ocular pain, trauma, or redness. Her medical history was significant for hypertension and dyslipidemia, both treated with oral medications. She had no previous history of diabetes mellitus or ocular surgery.
On examination, best-corrected visual acuity measured 6/6 in the right eye and 6/24 in the left eye. Intraocular pressures were within normal limits bilaterally. The anterior segment examination was unremarkable.
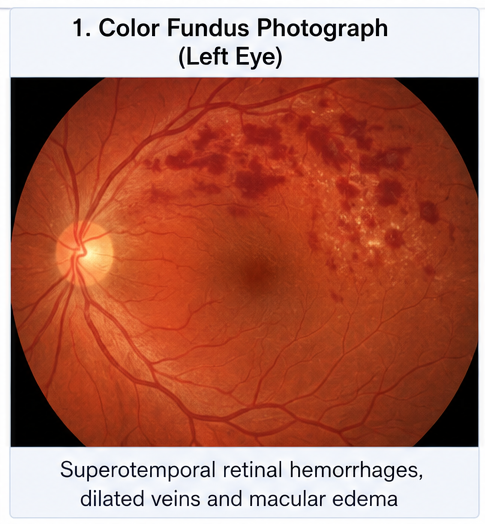
Dilated fundus examination of the left eye demonstrated multiple flame-shaped and dot-blot hemorrhages along the superotemporal retinal arcade with dilated tortuous retinal veins. The macula appeared thickened with loss of the normal foveal reflex, suggesting retinal edema. The right eye was normal.
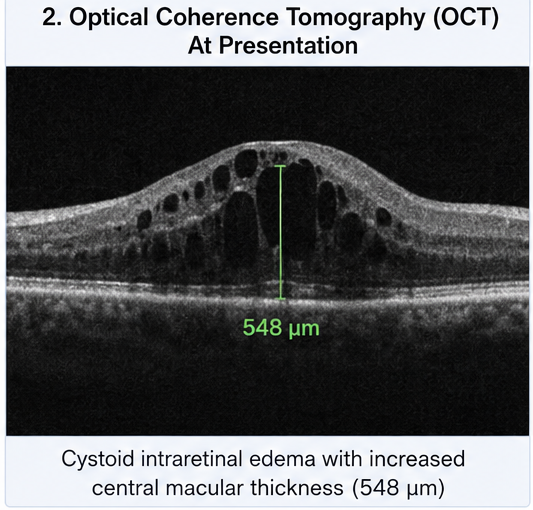
Optical coherence tomography revealed cystoid intraretinal fluid with disruption of the normal foveal contour and increased central macular thickness measuring 548 µm.
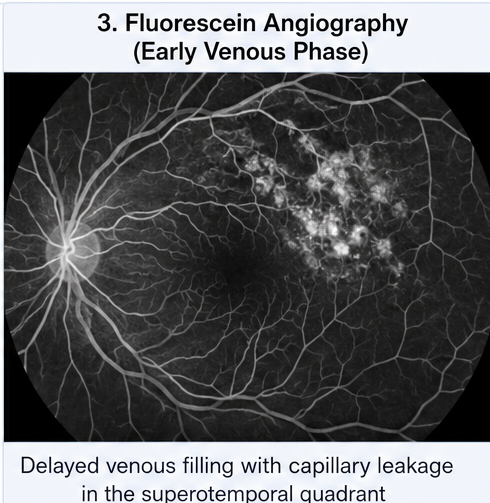
Fluorescein angiography demonstrated delayed venous filling with areas of capillary leakage in the affected quadrant, confirming branch retinal vein occlusion with macular edema.
Routine laboratory investigations, including complete blood count, fasting blood glucose, HbA1c, renal function tests, lipid profile, erythrocyte sedimentation rate, and coagulation profile, were within acceptable limits except for elevated serum cholesterol. Blood pressure measured 158/94 mmHg at presentation.
Based on the clinical examination and multimodal retinal imaging, a diagnosis of retinal edema secondary to branch retinal vein occlusion was established.
Management and Outcome
The patient was counseled regarding the disease process, treatment options, and the importance of systemic risk factor control. Blood pressure management was optimized in consultation with her physician.
Intravitreal aflibercept (2 mg/0.05 mL) was administered under aseptic conditions. The patient subsequently received two additional monthly loading doses according to standard treatment protocol.
She was advised regular OCT monitoring and educated regarding symptoms suggestive of worsening retinal ischemia or neovascular complications.
No injection-related complications, including endophthalmitis, retinal detachment, vitreous hemorrhage, or elevated intraocular pressure, were observed.
Follow-up
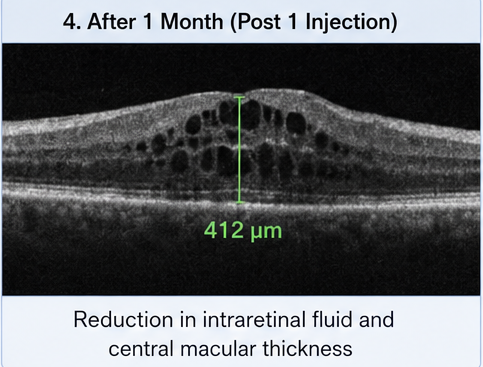
One Month
- Reduction in retinal thickness on OCT
- Improvement in visual acuity to 6/18
- Decrease in intraretinal cystic spaces
- No treatment-related adverse effects
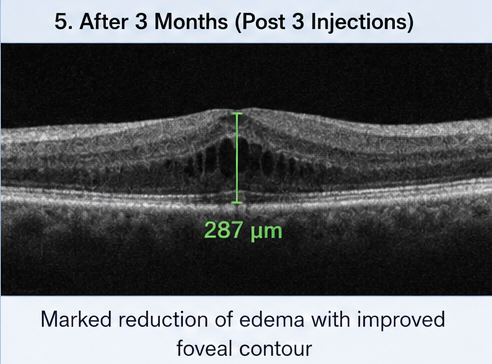
Three Months
- Visual acuity improved to 6/9
- Central macular thickness reduced to 287 µm
- Near-complete resolution of retinal edema
- Marked improvement in reading ability and daily visual function
Six Months
The patient maintained stable vision with complete anatomical resolution of retinal edema on OCT. No evidence of recurrent macular edema or retinal neovascularization was detected. Blood pressure remained well controlled, and continued ophthalmic follow-up was advised.
Discussion
Retinal edema remains one of the most significant causes of reversible visual impairment in retinal vascular diseases. In branch retinal vein occlusion, compression of a retinal vein at an arteriovenous crossing produces venous stasis, increased hydrostatic pressure, endothelial damage, and breakdown of the blood-retinal barrier. Subsequent leakage of plasma into the retinal tissue leads to macular edema and visual deterioration.
Optical coherence tomography is considered the gold standard for diagnosing and monitoring retinal edema because it provides high-resolution cross-sectional imaging of retinal architecture and quantitative assessment of central macular thickness. Fluorescein angiography complements OCT by identifying retinal ischemia, vascular leakage, and areas requiring laser treatment if indicated.
The introduction of anti-VEGF therapy has transformed the management of retinal edema. Agents such as aflibercept, ranibizumab, and bevacizumab inhibit VEGF-mediated vascular permeability, thereby reducing fluid accumulation and improving retinal anatomy. Multiple randomized clinical trials have demonstrated superior visual gains with anti-VEGF therapy compared with previous treatment modalities such as grid laser photocoagulation.
Although corticosteroid implants may be considered in selected patients, especially those with inadequate response to anti-VEGF therapy or contraindications to frequent injections, they carry increased risks of cataract formation and elevated intraocular pressure.
Systemic vascular risk factors including hypertension, diabetes, hyperlipidemia, and smoking significantly contribute to retinal vein occlusion. Therefore, multidisciplinary management addressing cardiovascular risk reduction is essential to minimize recurrence and prevent complications in the fellow eye.
This case highlights how prompt diagnosis using OCT and early initiation of intravitreal anti-VEGF therapy resulted in rapid anatomical improvement and excellent visual recovery.
Prognosis
The prognosis of retinal edema secondary to branch retinal vein occlusion has improved considerably with modern anti-VEGF therapy. Early treatment, regular OCT-guided monitoring, and appropriate management of systemic cardiovascular risk factors are associated with favorable long-term visual outcomes. Delayed diagnosis or untreated persistent edema may result in irreversible photoreceptor damage, retinal ischemia, and permanent visual impairment.
Conclusion
Retinal edema is a vision-threatening complication of branch retinal vein occlusion that requires prompt recognition and timely intervention. Comprehensive retinal examination supported by optical coherence tomography and fluorescein angiography enables accurate diagnosis and disease monitoring. Intravitreal anti-VEGF therapy remains the cornerstone of treatment, providing significant anatomical and functional improvement. Early management combined with optimal control of systemic vascular risk factors can preserve vision and improve patients' quality of life.
References
- Campochiaro PA, Clark WL, Boyer DS, et al. Intravitreal aflibercept for macular edema following branch retinal vein occlusion: The 24-week results of the VIBRANT study. Ophthalmology. 2015;122(3):538–544. https://pubmed.ncbi.nlm.nih.gov/25315663/
- Clark WL, Boyer DS, Heier JS, et al. Intravitreal aflibercept for macular edema following branch retinal vein occlusion: 52-week results of the VIBRANT study. Ophthalmology. 2016;123(2):330–336. https://pubmed.ncbi.nlm.nih.gov/26522708/
- Schmidt-Erfurth U, Garcia-Arumi J, Gerendas BS, et al. Guidelines for the Management of Retinal Vein Occlusion by the European Society of Retina Specialists (EURETINA). Ophthalmologica. 2019;242(3):123–162. https://pubmed.ncbi.nlm.nih.gov/31412332/
- Jonas JB, Monés J, Glacet-Bernard A, Coscas G. Retinal Vein Occlusions. Lancet. 2017;390(10098):1267–1278. https://doi.org/10.1016/S0140-6736(17)31452-4
- Oellers P, Mahmoud TH. Role of aflibercept for macular edema following branch retinal vein occlusion. Clinical Ophthalmology. 2016;10:859–869. https://pmc.ncbi.nlm.nih.gov/articles/PMC4789836/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge