Nutritional Vitamin D Deficiency Rickets Presenting with Bowing of Legs in a Child – A Case Report
OthersPage Navigation
Abstract
Rickets is a metabolic bone disorder occurring in growing children due to defective mineralization of the growth plate and newly formed bone. Vitamin D deficiency remains the most common cause of rickets worldwide, particularly in developing countries where inadequate sunlight exposure, poor dietary intake, and malnutrition continue to be significant public health concerns. Clinical manifestations include bone pain, delayed growth, skeletal deformities, muscle weakness, and impaired physical development.
We report the case of a 4-year-old boy who presented with progressive bowing of both lower limbs, delayed growth, and difficulty in walking. Clinical examination, biochemical investigations, and radiographic findings were consistent with nutritional vitamin D deficiency rickets. The child was treated with vitamin D supplementation, calcium therapy, nutritional counseling, and regular follow-up. Significant clinical and biochemical improvement was observed during follow-up. This case highlights the importance of early diagnosis and prompt treatment of nutritional rickets to prevent long-term skeletal complications and improve growth outcomes.
Introduction
Rickets is a childhood disorder characterized by impaired mineralization of the growth plate and osteoid tissue, resulting in skeletal deformities and growth disturbances. The condition primarily affects infants and young children during periods of rapid growth. Although various metabolic and genetic abnormalities can cause rickets, nutritional vitamin D deficiency remains the most common etiology globally.
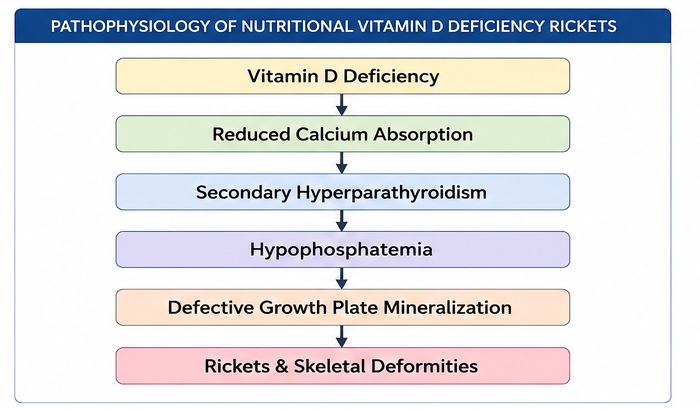
Vitamin D plays a crucial role in calcium and phosphorus homeostasis. Deficiency leads to decreased intestinal calcium absorption, secondary hyperparathyroidism, hypophosphatemia, and defective bone mineralization. Common risk factors include inadequate sunlight exposure, prolonged exclusive breastfeeding without supplementation, poor dietary intake, dark skin pigmentation, and malnutrition.
Typical clinical manifestations include:
• Bowing of legs
• Delayed growth
• Widening of wrists and ankles
• Bone pain
• Delayed motor milestones
• Muscle weakness
• Frontal bossing
• Rachitic rosary
Early recognition and treatment are essential to prevent permanent skeletal deformities and optimize growth and development.
Case Report
Patient History
A 4-year-old boy was brought to the pediatric outpatient department with complaints of:
• Progressive bowing of both legs
• Difficulty walking for the past six months
• Delayed growth compared to peers
• Easy fatigability during physical activity
The child's parents noticed gradual outward curvature of both lower limbs over the preceding year. The deformity became more prominent while walking and standing.
Dietary history revealed inadequate consumption of dairy products and vitamin D-rich foods. The child spent most of his time indoors and had limited exposure to sunlight.
There was no history of:
• Trauma
• Chronic kidney disease
• Chronic liver disease
• Recurrent fractures
• Seizures
• Developmental delay
Birth history was unremarkable. Immunization status was age-appropriate.
There was no family history of metabolic bone disease or hereditary rickets.
Clinical Examination
General examination revealed:
• Weight: 13 kg
• Height: 92 cm
• Mild growth retardation for age
• Alert and active child
Vital signs were stable:
• Pulse rate: 96 beats/minute
• Respiratory rate: 22 breaths/minute
• Blood pressure: 92/58 mmHg
• Temperature: Afebrile
Musculoskeletal examination showed:
• Bilateral genu varum (bowing of legs)
• Widening of wrists
• Prominent costochondral junctions (rachitic rosary)
• Mild frontal bossing
• Proximal muscle weakness
The child had a waddling gait but was able to walk independently.
No neurological abnormalities were detected.
Clinical Evaluation
Differential Diagnosis
The following differential diagnoses were considered:
• Nutritional vitamin D deficiency rickets
• Hypophosphatemic rickets
• Renal osteodystrophy
• Osteogenesis imperfecta
• Skeletal dysplasia
• Physiological bowing of legs
Investigations
Laboratory Evaluation
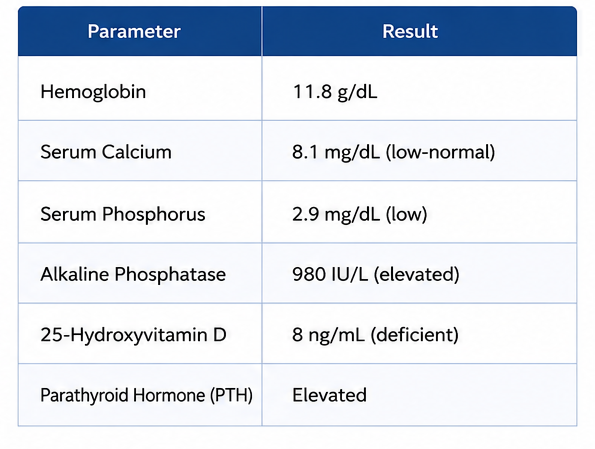
Routine laboratory investigations revealed:
• Hemoglobin: 11.8 g/dL
• White blood cell count: 7,800/mm³
• Platelet count: 295,000/mm³
Biochemical investigations showed:
• Serum calcium: 8.1 mg/dL (low-normal)
• Serum phosphorus: 2.9 mg/dL (low)
• Alkaline phosphatase: 980 IU/L (elevated)
• 25-hydroxyvitamin D: 8 ng/mL (deficient)
• Parathyroid hormone: Elevated
These findings were suggestive of vitamin D deficiency rickets.
Radiological Evaluation
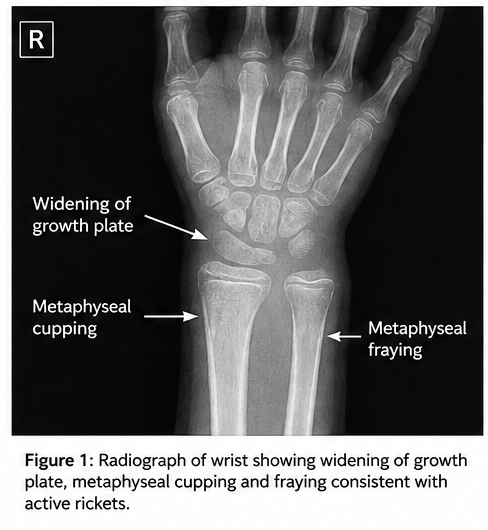
X-ray of both wrists demonstrated:
• Widening of growth plates
• Metaphyseal cupping
• Metaphyseal fraying
• Delayed mineralization
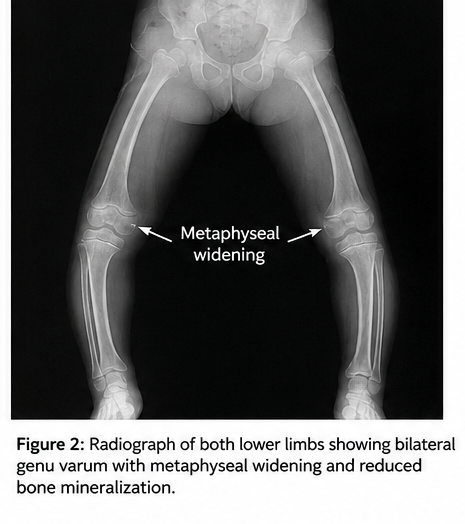
X-ray of both knees showed:
• Bowing deformity of lower limbs
• Metaphyseal widening
• Reduced bone density
These radiographic findings were characteristic of active rickets.
Diagnosis
Based on clinical features, biochemical abnormalities, and radiological findings, a diagnosis of: Nutritional Vitamin D Deficiency Rickets was established.
Management and Outcome
Medical Treatment
The child was started on:
• Oral vitamin D supplementation (60,000 IU weekly for six weeks)
• Oral calcium supplementation (500 mg elemental calcium daily)
• Dietary counseling for increased calcium intake
• Advice regarding regular sunlight exposure
Parents were educated regarding:
• Importance of vitamin D-rich foods
• Outdoor activities and sunlight exposure
• Medication compliance
Follow-Up
At 6 Weeks
Clinical assessment revealed:
• Improved activity levels
• Reduction in muscle weakness
• Better appetite
Laboratory investigations showed:
• Rising vitamin D levels
• Reduction in alkaline phosphatase levels
At 3 Months
The child demonstrated:
• Improved walking ability
• Increased physical activity
• Improved growth parameters
Repeat biochemical evaluation showed:
• Serum vitamin D within normal range
• Improved phosphorus levels
• Significant reduction in alkaline phosphatase
At 6 Months
Further improvement was noted:
• Decreased progression of bowing deformity
• Improved muscle strength
• Normal gait pattern
Radiographic examination demonstrated healing changes with improved mineralization and reduction in metaphyseal abnormalities.
Discussion
Nutritional vitamin D deficiency remains the most common cause of rickets worldwide despite the availability of effective preventive strategies. The condition results from inadequate vitamin D levels leading to impaired calcium and phosphorus metabolism and defective mineralization of growing bone.
Clinical Features
Common manifestations include:
• Bowing of legs
• Delayed growth
• Widened wrists and ankles
• Rachitic rosary
• Frontal bossing
• Delayed motor development
• Bone pain
The severity of symptoms depends on the degree and duration of vitamin D deficiency.
Diagnostic Evaluation
Diagnosis is established through a combination of:
• Clinical examination
• Biochemical investigations
• Radiological findings
Characteristic laboratory abnormalities include:
• Low vitamin D levels
• Elevated alkaline phosphatase
• Hypophosphatemia
• Secondary hyperparathyroidism
Radiographic findings such as metaphyseal cupping and fraying are highly suggestive of active rickets.
Treatment
Management primarily focuses on correcting vitamin D deficiency and restoring normal mineral metabolism.
Treatment strategies include:
• Vitamin D supplementation
• Calcium supplementation
• Nutritional counseling
• Increased sunlight exposure
Most children demonstrate rapid biochemical improvement following initiation of therapy, although correction of skeletal deformities may require a longer duration.
Prevention
Preventive measures include:
• Adequate sunlight exposure
• Vitamin D supplementation in high-risk children
• Balanced nutrition
• Public health education
Early intervention significantly reduces the risk of permanent skeletal deformities and growth impairment.
Prognosis
The prognosis of nutritional rickets is excellent when diagnosed and treated early. Most children achieve normalization of biochemical parameters and substantial improvement in skeletal abnormalities. Delayed diagnosis may result in persistent deformities requiring orthopedic intervention.
Conclusion
Nutritional vitamin D deficiency rickets remains an important pediatric health concern. This case highlights the classical presentation of rickets with bowing of legs, growth retardation, and characteristic biochemical and radiological abnormalities. Early diagnosis and prompt treatment with vitamin D and calcium supplementation resulted in significant clinical improvement and prevention of further skeletal complications. Awareness among parents and healthcare providers remains essential for timely identification and management of this preventable disorder.
References
- Munns CF, Shaw N, Kiely M, Specker BL, Thacher TD, Ozono K, et al. Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. J Clin Endocrinol Metab. 2016;101(2):394-415. https://pubmed.ncbi.nlm.nih.gov/26745253/
- Thacher TD, Fischer PR, Strand MA, Pettifor JM. Nutritional Rickets Around the World. Clin Pediatr (Phila). 2006;45(4):287-296. https://pubmed.ncbi.nlm.nih.gov/16703146/
- Pettifor JM. Nutritional Rickets: Deficiency of Vitamin D, Calcium, or Both? Am J Clin Nutr. 2004;80(6 Suppl):1725S-1729S. https://pubmed.ncbi.nlm.nih.gov/15585793/
- Carpenter TO, Shaw NJ, Portale AA, Ward LM, Abrams SA, Pettifor JM. Rickets. Nat Rev Dis Primers. 2017;3:17101. https://pubmed.ncbi.nlm.nih.gov/29222498/
- Elder CJ, Bishop NJ. Rickets. Lancet. 2014;383(9929):1665-1676. https://pubmed.ncbi.nlm.nih.gov/24725452/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge