Crohn's Disease Presenting with Ileocolonic Involvement in a Young Adult: A Case Report
OthersPage Navigation
Abstract
Crohn's disease (CD) is a chronic, relapsing inflammatory bowel disease characterized by transmural inflammation that can affect any segment of the gastrointestinal tract from the mouth to the anus. The disease commonly presents with abdominal pain, chronic diarrhea, weight loss, fatigue, and extraintestinal manifestations, significantly impairing quality of life. Early diagnosis through clinical evaluation, laboratory investigations, endoscopy, histopathology, and cross-sectional imaging is essential to prevent complications such as strictures, fistulas, abscesses, and malnutrition. We report the case of a 28-year-old man who presented with chronic abdominal pain, recurrent diarrhea, and progressive weight loss. Colonoscopy demonstrated patchy ulcerations involving the terminal ileum and ascending colon, while histopathological examination confirmed Crohn's disease. The patient responded well to corticosteroid induction therapy followed by maintenance treatment with azathioprine and lifestyle modifications. Significant clinical and biochemical remission was achieved during six months of follow-up. This case highlights the importance of early recognition, multidisciplinary management, and long-term monitoring in achieving favorable outcomes in Crohn's disease.
Introduction
Crohn's disease is a chronic immune-mediated inflammatory bowel disease characterized by discontinuous ("skip") lesions and transmural inflammation of the gastrointestinal tract. Although the terminal ileum and colon are the most commonly affected sites, inflammation may occur anywhere from the oral cavity to the perianal region. The exact etiology remains multifactorial, involving genetic susceptibility, immune dysregulation, environmental factors, alterations in gut microbiota, and impaired intestinal barrier function.
The incidence of Crohn's disease has increased globally over the past two decades, particularly in newly industrialized countries. Patients usually present during adolescence or early adulthood with recurrent abdominal pain, chronic diarrhea, rectal bleeding, weight loss, fatigue, and nutritional deficiencies. Delayed diagnosis may lead to intestinal strictures, fistula formation, bowel obstruction, abscesses, growth impairment in children, and increased need for surgical intervention.
Current management focuses on inducing remission, maintaining long-term disease control, preventing complications, improving nutritional status, and enhancing quality of life using a combination of pharmacological therapy, nutritional support, and regular surveillance.
Case Report
A 28-year-old man presented to the gastroenterology outpatient department with intermittent crampy abdominal pain and loose stools for the previous eight months. He reported passing five to six loose stools daily, occasionally mixed with mucus, along with loss of appetite and an unintentional weight loss of approximately 8 kg over six months. He also complained of generalized fatigue and intermittent low-grade fever. There was no history of recent travel, tuberculosis, or prolonged antibiotic use.
On physical examination, the patient appeared mildly pale and underweight but was hemodynamically stable. Mild tenderness was present over the right lower quadrant without guarding or rigidity. No palpable abdominal mass was detected. Perianal examination was unremarkable.
Laboratory investigations revealed hemoglobin of 10.8 g/dL, leukocyte count of 12,100 cells/mm³, elevated C-reactive protein of 38 mg/L, erythrocyte sedimentation rate of 48 mm/hour, serum albumin of 3.1 g/dL, and fecal calprotectin of 760 µg/g. Stool cultures were negative for bacterial pathogens and parasites.
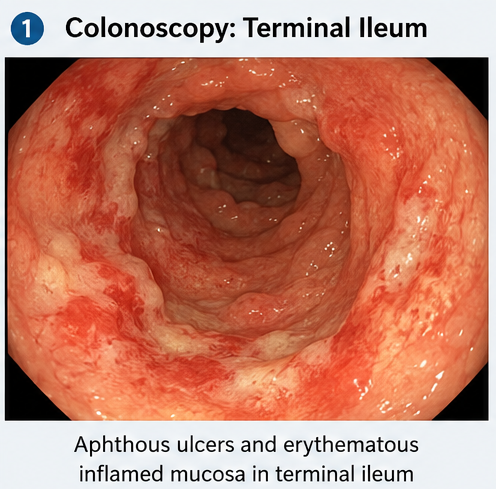
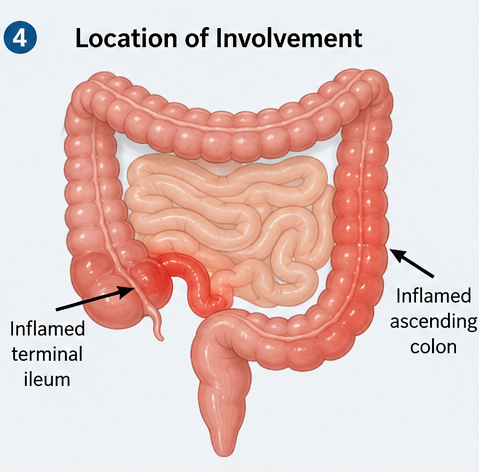
Colonoscopy demonstrated multiple aphthous ulcers, deep longitudinal ulcerations, and patchy areas of inflamed mucosa involving the terminal ileum and ascending colon with intervening normal mucosa.
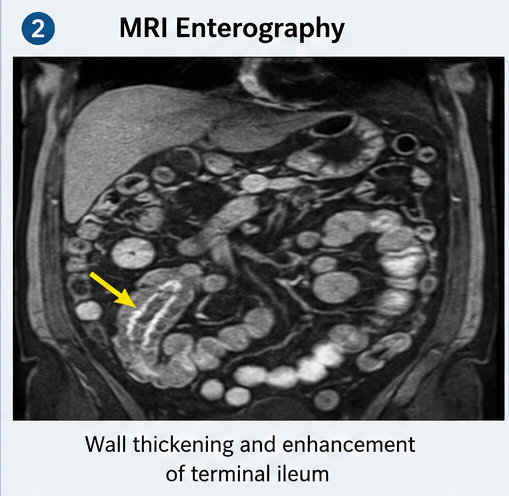
Magnetic resonance enterography confirmed active inflammation of the terminal ileum without evidence of fistula or abscess formation.
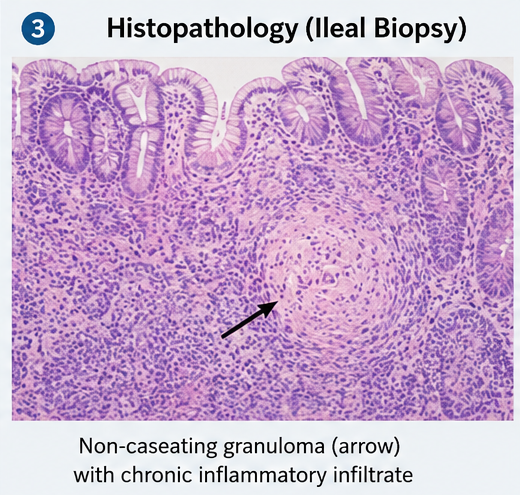
Histopathological examination of biopsy specimens showed chronic active inflammation with focal crypt distortion, transmural inflammatory infiltrates, and non-caseating granulomas, consistent with Crohn's disease.
Based on the clinical presentation, endoscopic findings, imaging, and histopathological examination, a diagnosis of moderate ileocolonic Crohn's disease was established.
Management and Outcome
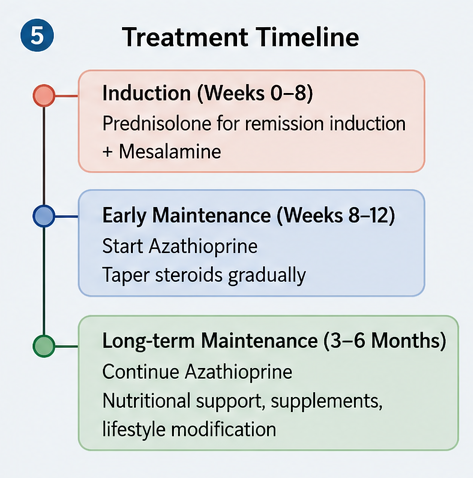
The patient was admitted for initiation of therapy and nutritional optimization. Oral prednisolone was started to induce remission, along with mesalamine for symptomatic control during the early phase of treatment. Azathioprine was initiated as a steroid-sparing immunomodulator after appropriate baseline evaluation. Iron supplementation, folic acid, vitamin B12, calcium, and vitamin D replacement were prescribed to correct nutritional deficiencies.
A dietitian recommended a high-protein, low-residue diet during active disease, adequate hydration, and avoidance of foods that aggravated gastrointestinal symptoms. Smoking cessation counseling was provided despite the patient being an occasional smoker, as tobacco use is associated with worse disease outcomes.
The patient showed gradual clinical improvement over the following weeks, with reduction in abdominal pain and stool frequency. Corticosteroids were gradually tapered while azathioprine was continued for maintenance therapy. No adverse drug reactions or infectious complications occurred during treatment.
Follow-up
One Month
- Stool frequency reduced to two to three times daily.
- Significant improvement in abdominal pain and appetite.
- Body weight increased by 2 kg.
- C-reactive protein declined substantially.
Three Months
- Complete resolution of diarrhea.
- Weight gain of approximately 5 kg from baseline.
- Hemoglobin and serum albumin improved.
- Fecal calprotectin demonstrated marked reduction, indicating decreased intestinal inflammation.
Six Months
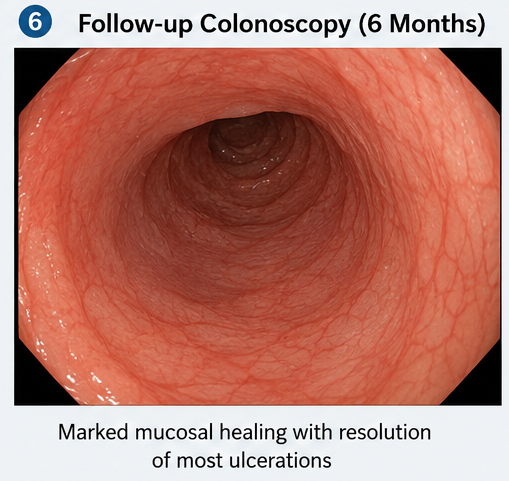
Clinical remission was maintained with azathioprine therapy. Follow-up colonoscopy demonstrated marked mucosal healing with resolution of most ulcerations and significant reduction in inflammatory activity. The patient resumed routine daily activities without recurrence of symptoms and remained under regular gastroenterology follow-up.
Discussion
Crohn's disease is a lifelong inflammatory disorder characterized by periods of relapse and remission. Unlike ulcerative colitis, Crohn's disease affects the entire thickness of the bowel wall and frequently produces discontinuous areas of inflammation separated by healthy bowel segments. This transmural inflammation predisposes patients to strictures, fistulas, abscesses, and intestinal perforation.
The diagnosis requires integration of clinical findings with laboratory markers, endoscopic evaluation, histopathology, and radiological imaging. Elevated fecal calprotectin serves as a useful non-invasive biomarker of intestinal inflammation and helps distinguish inflammatory bowel disease from functional gastrointestinal disorders. Colonoscopy with biopsy remains the diagnostic gold standard, while magnetic resonance enterography provides excellent assessment of small bowel involvement and extraintestinal complications.
The therapeutic approach depends on disease severity, location, and presence of complications. Corticosteroids remain effective for induction of remission but should not be used for long-term maintenance because of significant adverse effects. Immunomodulators such as azathioprine and methotrexate help maintain remission and reduce steroid dependence. Biologic therapies targeting tumor necrosis factor-alpha, integrins, or interleukin-12/23 pathways have transformed the management of moderate-to-severe Crohn's disease and are recommended for patients with refractory or high-risk disease.
Nutritional management plays an essential role because chronic intestinal inflammation frequently results in protein-energy malnutrition, anemia, vitamin deficiencies, and impaired bone health. Regular monitoring of nutritional status, vaccination, infection screening, and colorectal cancer surveillance are important components of long-term care.
This case demonstrates that prompt diagnosis and early institution of evidence-based therapy can achieve sustained remission, promote mucosal healing, and improve overall quality of life while reducing the risk of disease-related complications.
Prognosis
The prognosis of Crohn's disease varies depending on disease location, severity, response to treatment, and patient adherence. Early diagnosis combined with appropriate medical therapy significantly improves long-term outcomes and reduces hospitalization and surgery rates. Although Crohn's disease remains incurable, advances in immunomodulatory and biologic therapies have substantially improved disease control, allowing many patients to achieve prolonged clinical and endoscopic remission. Lifelong follow-up is necessary because relapses and complications may occur despite successful treatment.
Conclusion
Crohn's disease is a chronic inflammatory bowel disorder requiring early diagnosis and comprehensive multidisciplinary management. Careful clinical evaluation, endoscopy with histopathological confirmation, laboratory monitoring, and cross-sectional imaging are fundamental for accurate diagnosis and treatment planning. Timely initiation of corticosteroids for remission induction, appropriate maintenance therapy with immunomodulators or biologics, nutritional optimization, and regular follow-up can achieve sustained remission, minimize complications, and significantly improve long-term patient outcomes.
References
- Torres J, Bonovas S, Doherty G, et al. ECCO Guidelines on Therapeutics in Crohn's Disease: Medical Treatment. Journal of Crohn's and Colitis. 2020;14(1):4-22. https://pubmed.ncbi.nlm.nih.gov/31711158/
- Feuerstein JD, Ho EY, Shmidt E, et al. AGA Clinical Practice Guidelines on the Medical Management of Moderate to Severe Luminal and Fistulizing Crohn's Disease. Gastroenterology. 2021;160(7):2496-2508. https://pubmed.ncbi.nlm.nih.gov/33910001/
- Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. Crohn's disease. The Lancet. 2017;389(10080):1741-1755. https://pubmed.ncbi.nlm.nih.gov/27815109/
- Gomollón F, Dignass A, Annese V, et al. 3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn's Disease. Journal of Crohn's and Colitis. 2017;11(1):3-25. https://pubmed.ncbi.nlm.nih.gov/27660341/
- Lichtenstein GR, Loftus EV Jr, Isaacs KL, et al. ACG Clinical Guideline: Management of Crohn's Disease in Adults. American Journal of Gastroenterology. 2018;113(4):481-517. https://pubmed.ncbi.nlm.nih.gov/29610508/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge