Nasal Valve Collapse Presenting as Chronic Nasal Obstruction: A Case Report
OthersPage Navigation
Abstract
Nasal valve collapse (NVC) is an underrecognized yet important cause of chronic nasal obstruction. It may occur due to congenital weakness, trauma, aging, previous nasal surgery, or connective tissue disorders. The internal nasal valve represents the narrowest segment of the upper airway and contributes significantly to nasal airflow resistance. Failure to identify nasal valve dysfunction often leads to persistent symptoms despite medical treatment. We report the case of a 45-year-old man who presented with progressive unilateral nasal obstruction, difficulty breathing during exercise, nocturnal mouth breathing, and poor sleep quality for over one year. Clinical examination demonstrated inspiratory collapse of the right nasal valve with a positive Cottle maneuver. Nasal endoscopy excluded significant septal deviation or sinonasal pathology. Computed tomography revealed mild septal deviation without evidence of chronic sinus disease. The patient underwent functional septorhinoplasty with internal nasal valve reconstruction using spreader grafts. Marked improvement in nasal airflow and quality of life was observed during follow-up. This case highlights the importance of recognizing nasal valve collapse as a distinct cause of nasal obstruction and emphasizes the role of timely surgical intervention in restoring normal nasal function.
Introduction
Nasal obstruction is one of the most common complaints encountered in otolaryngology practice. Although septal deviation, allergic rhinitis, and turbinate hypertrophy account for the majority of cases, nasal valve collapse remains a frequently overlooked etiology. The internal nasal valve, formed by the angle between the upper lateral cartilage and the nasal septum, is the narrowest portion of the nasal airway and contributes nearly half of total nasal airflow resistance. Even minor structural compromise may significantly impair nasal breathing.
Nasal valve collapse may be static or dynamic and is commonly associated with facial trauma, previous rhinoplasty, congenital cartilage weakness, or age-related loss of structural support. Diagnosis relies primarily on careful clinical examination supplemented by nasal endoscopy and imaging when indicated. Conservative measures such as nasal dilator strips may provide temporary relief; however, definitive management often requires functional nasal valve reconstruction. Early recognition is essential to improve patient outcomes and avoid unnecessary prolonged medical therapy.
Case Report
A 45-year-old man presented to the otolaryngology outpatient department with progressive right-sided nasal obstruction for approximately one year. He reported increasing difficulty breathing through the nose, particularly during exercise and at night, resulting in habitual mouth breathing and disturbed sleep. The patient denied recurrent sinus infections, epistaxis, facial pain, anosmia, or allergic symptoms. There was a remote history of minor nasal trauma sustained during recreational sports nearly five years earlier, which had not required medical attention.
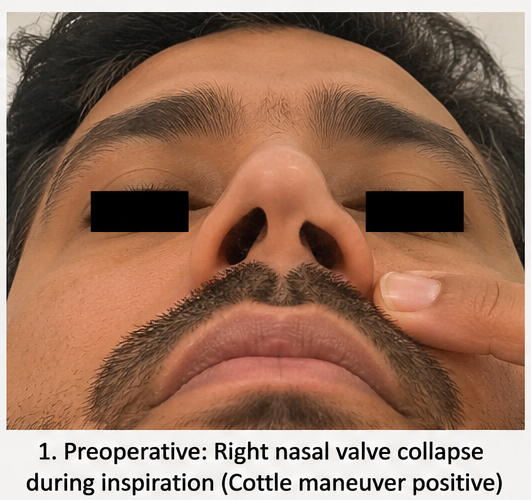
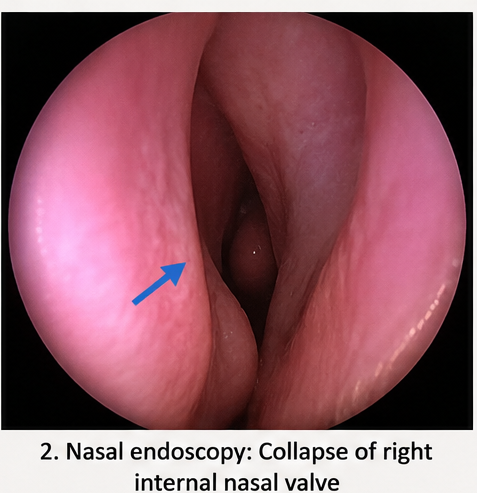
General physical examination was unremarkable. Facial symmetry was preserved, and no obvious external nasal deformity was evident. During quiet inspiration, partial collapse of the right nasal sidewall was observed, becoming more pronounced during deep inspiration. The Cottle maneuver produced immediate improvement in nasal airflow, strongly suggesting internal nasal valve dysfunction. Anterior rhinoscopy demonstrated mild septal deviation without significant inferior turbinate hypertrophy. Diagnostic nasal endoscopy confirmed dynamic collapse of the right internal nasal valve while excluding nasal polyps, chronic rhinosinusitis, masses, or other obstructive lesions.
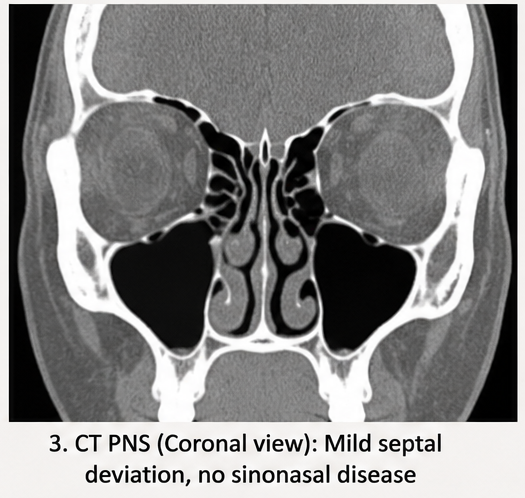
Routine laboratory investigations, including complete blood count, coagulation profile, renal function tests, and inflammatory markers, were within normal limits. Computed tomography of the paranasal sinuses demonstrated mild rightward septal deviation with preserved sinus aeration and no evidence of sinonasal inflammatory disease or bony abnormality.
Based on the patient's clinical findings, dynamic examination, and radiological evaluation, a diagnosis of symptomatic right internal nasal valve collapse was established.
Management and Outcome
Initial conservative management included saline nasal irrigation, external nasal dilator strips during sleep, and avoidance of environmental irritants. Despite six weeks of treatment, the patient continued to experience significant nasal obstruction affecting daily activities and sleep quality.
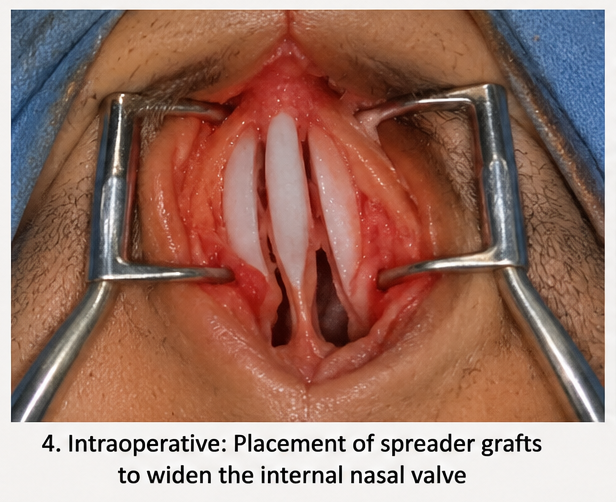
Following detailed counseling regarding available treatment options, the patient underwent functional septorhinoplasty under general anesthesia. The procedure included correction of the mild septal deviation, placement of bilateral spreader grafts to widen the internal nasal valve angle, and reinforcement of the upper lateral cartilages. Intraoperative findings confirmed weakened upper lateral cartilage contributing to dynamic inspiratory collapse.
The postoperative period was uneventful. Nasal packing was removed on the second postoperative day, and silicone splints were removed after one week. The patient was advised to continue saline nasal irrigation and avoid strenuous physical activity for four weeks.
Follow-up
Two Weeks
- Significant reduction in nasal obstruction
- Improved nasal airflow
- Minimal postoperative edema
- Well-healed surgical incision
One Month
- Resolution of nocturnal mouth breathing
- Improved exercise tolerance
- Marked improvement in sleep quality
- NOSE (Nasal Obstruction Symptom Evaluation) score improved substantially
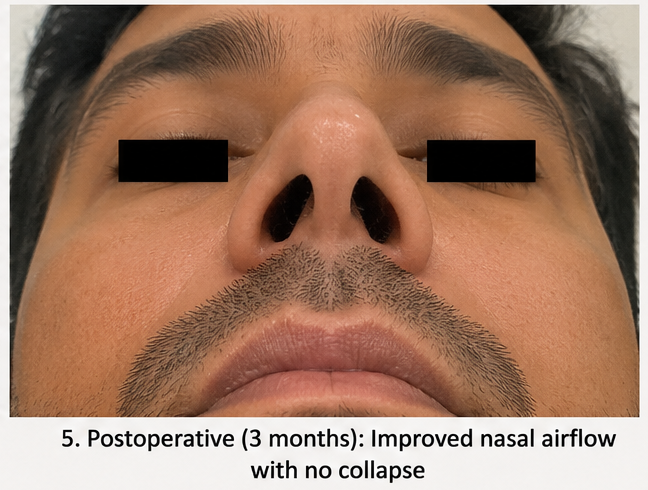
Three Months
The patient remained asymptomatic with excellent bilateral nasal airflow. Dynamic collapse was no longer observed during inspiration, and cosmetic appearance remained unchanged. No surgical complications or recurrence of symptoms were noted.
Discussion
Nasal valve collapse is increasingly recognized as a major structural cause of persistent nasal obstruction. Because symptoms frequently overlap with septal deviation and allergic rhinitis, diagnosis is often delayed. Careful observation during inspiration, together with simple bedside maneuvers such as the Cottle or modified Cottle test, remains highly valuable for identifying functional valve compromise.
The internal nasal valve normally forms an angle of approximately 10–15 degrees. Narrowing of this angle or weakening of the supporting cartilages increases airflow resistance according to fluid dynamic principles, resulting in progressive inspiratory collapse and impaired nasal breathing. Previous trauma, rhinoplasty, congenital anatomical variation, and age-related cartilage degeneration are among the most common predisposing factors.
Although imaging studies help exclude associated pathology, nasal valve collapse remains primarily a clinical diagnosis. Functional nasal surgery aims to restore adequate structural support while preserving nasal aesthetics. Among available surgical techniques, spreader grafts remain the gold standard for reconstruction of the internal nasal valve because they increase the valve angle and improve airflow. Alternative techniques include butterfly grafts, alar batten grafts, flaring sutures, and bioabsorbable lateral wall implants, selected according to the underlying anatomical defect.
Patient-reported outcome measures, particularly the NOSE score, have consistently demonstrated significant postoperative improvement following functional nasal valve reconstruction. Long-term studies report durable symptomatic relief with low complication rates when appropriate surgical techniques are employed. This case illustrates that even subtle structural abnormalities may produce substantial functional impairment and should be considered in patients with chronic nasal obstruction unresponsive to medical therapy.
Prognosis
Patients undergoing appropriately selected functional nasal valve reconstruction generally experience excellent long-term outcomes with sustained improvement in nasal airflow, sleep quality, exercise tolerance, and overall quality of life. Early diagnosis and individualized surgical planning minimize recurrence while preserving both nasal function and facial aesthetics.
Conclusion
Nasal valve collapse should be considered in patients presenting with persistent nasal obstruction despite appropriate medical management. A thorough clinical examination, including assessment for dynamic nasal valve dysfunction and supportive endoscopic evaluation, is essential for establishing the diagnosis. Functional septorhinoplasty with internal nasal valve reconstruction remains an effective treatment option for symptomatic patients who fail conservative therapy. Early recognition and timely surgical intervention can significantly improve nasal airflow, patient satisfaction, and long-term functional outcomes.
References
-
Rhee JS, Weaver EM, Park SS, et al. Clinical Consensus Statement: Diagnosis and Management of Nasal Valve Compromise. Otolaryngol Head Neck Surg. 2010;143(1):48–59. https://pubmed.ncbi.nlm.nih.gov/20620619/
-
Ishii LE, Tollefson TT, Basura GJ, et al. Clinical Practice Guideline: Improving Nasal Form and Function after Rhinoplasty. Otolaryngol Head Neck Surg. 2017;156(2 Suppl):S1–S30. https://pubmed.ncbi.nlm.nih.gov/28145823/
-
Most SP. Trends in Functional Rhinoplasty. Arch Facial Plast Surg. 2008;10(6):410–413. https://doi.org/10.1001/archfaci.10.6.410
-
Sidle DM, Stolovitzky JP. Surgical Management of Nasal Valve Collapse. Facial Plast Surg Clin North Am. 2022;30(1):73–84. https://doi.org/10.1016/j.fsc.2021.08.008
-
Ishii LE, Tollefson TT, Basura GJ, et al. Diagnosis and Management of Nasal Valve Collapse. Otolaryngol Clin North Am. 2021;54(5):919–933. https://doi.org/10.1016/j.otc.2021.05.006
-
Fraser L, Kelly G. An Evidence-Based Approach to Nasal Valve Obstruction. Clin Otolaryngol. 2009;34(5):447–454. https://doi.org/10.1111/j.1749-4486.2009.02016.x
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge