Pleural Effusion: Clinical Presentation, Diagnostic Evaluation, Therapeutic Thoracentesis, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Pleural effusion is a common clinical condition characterized by the abnormal accumulation of fluid within the pleural space. It may result from a wide range of infectious, malignant, cardiac, hepatic, renal, and inflammatory disorders. Patients often present with dyspnea, cough, chest discomfort, and reduced exercise tolerance, with symptom severity depending on the volume of fluid accumulation and the underlying etiology.
Accurate diagnosis requires a systematic approach involving clinical assessment, radiological imaging, and pleural fluid analysis. Diagnostic thoracentesis remains the cornerstone for determining the cause of pleural effusion and guiding appropriate management.
We present the case of a 58-year-old male who presented with progressive shortness of breath, dry cough, and right-sided chest heaviness. Clinical examination and radiological investigations revealed a moderate right-sided pleural effusion. Pleural fluid analysis demonstrated an exudative lymphocyte-predominant effusion consistent with tuberculous pleuritis. Therapeutic thoracentesis followed by anti-tubercular therapy resulted in complete clinical and radiological recovery.
This case highlights the importance of early recognition, comprehensive diagnostic evaluation, and timely intervention in achieving favorable outcomes in patients with pleural effusion.
Introduction
Pleural effusion refers to the abnormal accumulation of fluid within the pleural cavity. Under normal physiological conditions, a small amount of pleural fluid lubricates the pleural surfaces and facilitates lung expansion during respiration. Various pathological processes can disrupt the balance between pleural fluid formation and absorption, resulting in fluid accumulation.
Pleural effusions are commonly encountered in clinical practice and may arise from both pulmonary and extrapulmonary disorders. The condition may significantly impair respiratory function and quality of life, particularly when large fluid volumes accumulate.
Common causes of pleural effusion include:
• Tuberculosis
• Pneumonia
• Malignancy
• Congestive heart failure
• Liver cirrhosis
• Nephrotic syndrome
• Pulmonary embolism
• Connective tissue disorders
Risk factors include:
• Advanced age
• Smoking history
• Chronic lung disease
• Immunosuppression
• Previous tuberculosis exposure
• Malignancy
• Chronic cardiac disease
Pathophysiological mechanisms involved in pleural effusion formation include:
• Increased hydrostatic pressure
• Reduced oncotic pressure
• Increased capillary permeability
• Impaired lymphatic drainage
• Pleural inflammation
• Direct pleural infiltration by malignancy
Common clinical manifestations include:
• Progressive dyspnea
• Dry or productive cough
• Chest pain
• Chest heaviness
• Fatigue
• Reduced exercise tolerance
Prompt diagnosis and treatment are essential to prevent complications and address the underlying disease process.
Case Report
Patient History
A 58-year-old male presented to the respiratory medicine outpatient department with complaints of:
• Progressive shortness of breath for 3 weeks
• Dry cough for 2 weeks
• Right-sided chest heaviness
• Fatigue and generalized weakness
• Reduced exercise tolerance
The patient reported gradual worsening of breathlessness over several weeks. Initially, symptoms occurred during exertion but later interfered with routine daily activities.
Additional history revealed:
• Loss of appetite for 1 month
• Weight loss of approximately 3 kg over 6 weeks
• No hemoptysis
• No fever at presentation
Past medical history revealed:
• Hypertension controlled with medication
• Former smoker (20 pack-years)
• No previous history of tuberculosis
There was no history of:
• Recent chest trauma
• Previous thoracic surgery
• Known malignancy
• Chronic liver disease
• Congestive cardiac failure
Clinical Examination
General Examination
• Blood pressure: 132/84 mmHg
• Pulse rate: 88/min
• Respiratory rate: 22/min
• Temperature: Afebrile
• Oxygen saturation: 95% on room air
The patient appeared mildly dyspneic but was hemodynamically stable.
Respiratory Examination
Inspection revealed:
• Reduced movement of the right hemithorax
• Mild respiratory distress
Palpation demonstrated:
• Reduced chest expansion on the right side
• Decreased tactile vocal fremitus
Percussion findings included:
• Stony dull note over the right lower lung zones
Auscultation revealed:
• Decreased breath sounds over the right infra-axillary and infrascapular regions
• Reduced vocal resonance
• No wheeze or crackles
The remainder of systemic examination was unremarkable.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Tuberculous pleural effusion
• Malignant pleural effusion
• Parapneumonic effusion
• Congestive cardiac failure-related effusion
• Pulmonary embolism
The combination of dyspnea, unilateral pleural fluid accumulation, and constitutional symptoms strongly suggested an exudative pleural effusion.
Investigations
Laboratory Evaluation
Routine investigations demonstrated:
• Hemoglobin: 12.8 g/dL
• Total leukocyte count: 8,900/mm³
• ESR: 42 mm/hr
• Renal function tests: Normal
• Liver function tests: Normal
• Blood glucose: Normal
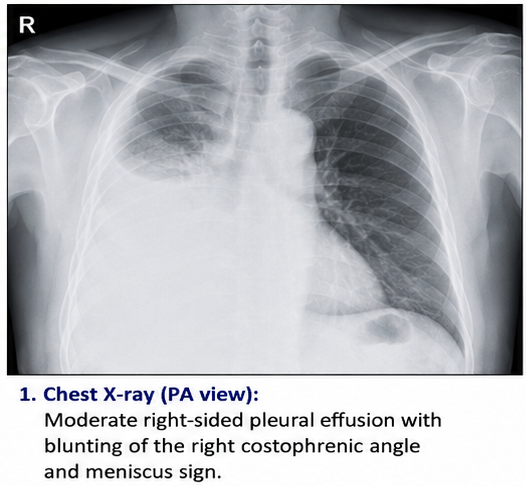
Chest Radiography
Chest X-ray demonstrated:
• Moderate right-sided pleural effusion
• Blunting of the right costophrenic angle
• Meniscus sign
• No obvious pulmonary mass lesion
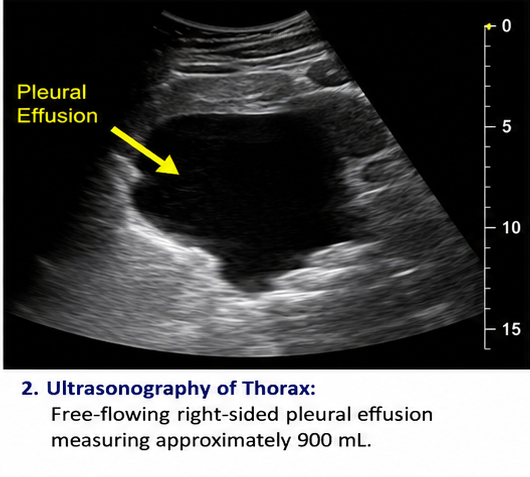
Ultrasonography of Thorax
Findings included:
• Approximately 900 mL pleural fluid
• Free-flowing effusion
• No loculations
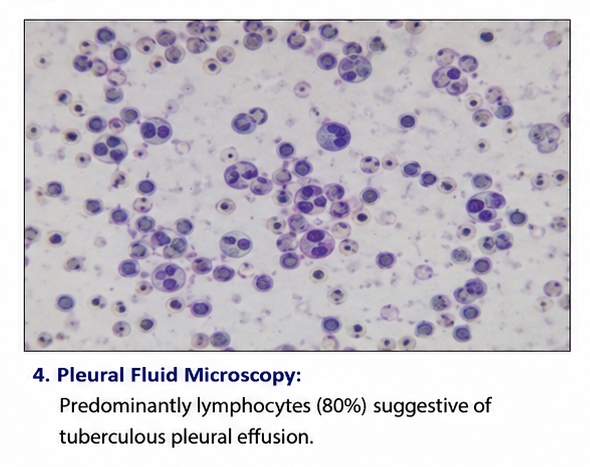
Diagnostic Thoracentesis
Pleural fluid analysis revealed:
• Straw-colored fluid
• Protein: 4.5 g/dL
• Elevated LDH
• Lymphocyte predominance (80%)
• ADA: 65 U/L
• Cytology negative for malignant cells
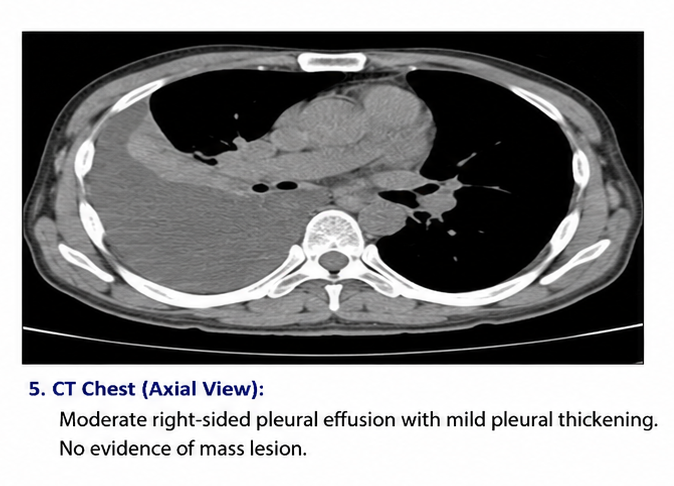
Computed Tomography (CT) Chest
CT findings included:
• Moderate right-sided pleural effusion
• Mild pleural thickening
• No lung mass
• No mediastinal lymphadenopathy
Diagnosis
Based on clinical examination, imaging studies, and pleural fluid analysis, a diagnosis of: Right-Sided Tuberculous Exudative Pleural Effusion was established.
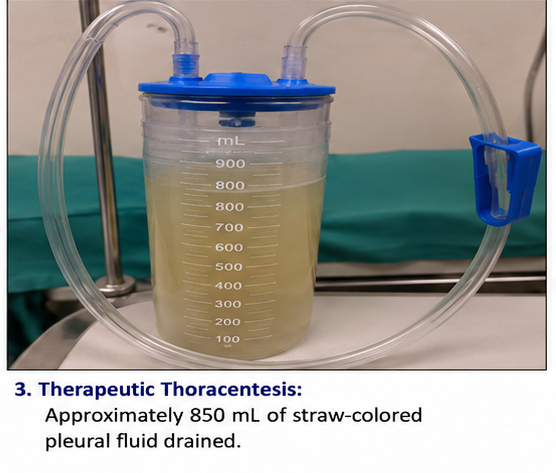
Management and Outcome
Initial Management
The patient underwent ultrasound-guided therapeutic thoracentesis.
Approximately 850 mL of pleural fluid was drained, resulting in immediate symptomatic improvement.
Following confirmation of tuberculous pleuritis, anti-tubercular therapy was initiated.
Treatment included:
• Standard anti-tubercular regimen
• Nutritional support
• Pulmonary rehabilitation advice
• Follow-up imaging
Follow-Up and Clinical Course
At 1 Week
• Significant improvement in dyspnea
• No procedural complications
• Improved oxygenation
At 1 Month
• Marked reduction in pleural fluid volume
• Improved appetite
• Increased exercise tolerance
At 3 Months
• Near-complete radiological resolution
• Weight gain of 2 kg
• No respiratory symptoms
At 6 Months
• Complete clinical recovery
• Normal daily activities resumed
• Chest radiograph showed complete resolution
• No recurrence of pleural effusion
Discussion
Pathophysiology
Pleural effusions develop when pleural fluid formation exceeds pleural fluid absorption. Multiple mechanisms contribute to this imbalance.
Key pathological processes include:
• Increased vascular permeability
• Pleural inflammation
• Impaired lymphatic drainage
• Increased hydrostatic pressure
• Reduced plasma oncotic pressure
Tuberculous pleuritis results from a delayed hypersensitivity reaction to Mycobacterium tuberculosis antigens within the pleural space, leading to lymphocyte-rich exudative effusion formation.
Epidemiology
Important epidemiological features include:
• Pleural effusion affects millions of individuals worldwide annually
• Tuberculosis remains a leading cause in developing countries
• Incidence increases with advancing age
• Smoking increases the risk of associated pulmonary disorders
• Exudative effusions are commonly linked to infection and malignancy
Clinical Manifestations
Patients with pleural effusion commonly present with:
• Progressive dyspnea
• Chest discomfort
• Cough
• Fatigue
• Reduced exercise capacity
Characteristic physical findings include:
• Reduced chest expansion
• Stony dull percussion note
• Decreased breath sounds
• Reduced vocal fremitus
Severity often correlates with the volume of pleural fluid.
Diagnostic Considerations
Diagnosis is based on:
- Detailed history
- Physical examination
- Chest radiography
- Thoracic ultrasonography
- Pleural fluid analysis
- CT imaging when indicated
Pleural fluid analysis remains the most important diagnostic tool for determining the underlying cause.
Treatment Modalities
Conservative Management
Management depends on the etiology and severity of symptoms.
Options include:
• Observation in small asymptomatic effusions
• Treatment of underlying disease
• Antibiotics when indicated
• Diuretics for transudative causes
Therapeutic Thoracentesis
Benefits include:
• Rapid symptom relief
• Improved lung expansion
• Diagnostic information
• Prevention of complications
Disease-Specific Treatment
Tuberculous pleural effusion requires:
• Anti-tubercular therapy
• Nutritional optimization
• Regular follow-up imaging
Complications
Potential complications include:
• Empyema
• Pleural fibrosis
• Trapped lung
• Respiratory failure
• Recurrent pleural effusion
Early diagnosis significantly reduces morbidity.
Prognosis
The prognosis depends primarily on the underlying cause.
Factors influencing outcomes include:
• Etiology of pleural effusion
• Timeliness of diagnosis
• Adequacy of treatment
• Patient compliance
• Presence of comorbidities
Tuberculous pleural effusions generally have an excellent prognosis when diagnosed early and treated appropriately.
Conclusion
Pleural effusion is a common clinical condition that may arise from a variety of infectious, inflammatory, malignant, and systemic disorders. Careful clinical assessment combined with imaging and pleural fluid analysis is essential for establishing an accurate diagnosis. This case demonstrates the successful management of tuberculous pleural effusion through therapeutic thoracentesis and anti-tubercular therapy, resulting in complete clinical and radiological recovery. Early recognition, prompt intervention, and appropriate treatment remain critical for achieving favorable outcomes and preventing long-term complications.
References
- Roberts ME, Rahman NM, Maskell NA, et al. British Thoracic Society Guideline for pleural disease. Thorax. 2023;78(11):1143-1156. https://pubmed.ncbi.nlm.nih.gov/37553157/
- Krishna R, Rudrappa M. Pleural Effusion. StatPearls. Treasure Island (FL): StatPearls Publishing; 2024. https://www.ncbi.nlm.nih.gov/books/NBK448189/
- Karkhanis VS, Joshi JM. Pleural effusion: diagnosis, treatment, and management. Open Access Emergency Medicine. 2012;4:31-52. https://pmc.ncbi.nlm.nih.gov/articles/PMC4753987/
- Jany B, Welte T. Pleural effusion in adults—etiology, diagnosis, and treatment. Deutsches Ärzteblatt International. 2019;116(21):377-386. https://pmc.ncbi.nlm.nih.gov/articles/PMC6647819/
- Porcel JM. Pleural fluid analysis: Are Light’s criteria still relevant after half a century? Clinics in Chest Medicine. 2021;42(4):599-609. https://pubmed.ncbi.nlm.nih.gov/34774168/
- Light RW. The Light criteria: the beginning and why they are useful 40 years later. Clinics in Chest Medicine. 2013;34(1):21-26. https://pubmed.ncbi.nlm.nih.gov/23411053/
- Antonangelo L, Faria CS, Sales RK. Tuberculous pleural effusion: diagnosis and management. Expert Review of Respiratory Medicine. 2019;13(8):747-759. https://pubmed.ncbi.nlm.nih.gov/31246102/
- Gopi A, Madhavan SM, Sharma SK, Sahn SA. Diagnosis and treatment of tuberculous pleural effusion in 2006. Chest. 2007;131(3):880-889. https://pubmed.ncbi.nlm.nih.gov/17356108/
- Cascio CML, Kaul V, Dhooria S, et al. Diagnosis of tuberculous pleural effusions: A review. Respiratory Medicine. 2021;188:106607. https://pubmed.ncbi.nlm.nih.gov/34536698/
- Christopher DJ, et al. Pleural effusion guidelines from ICS and NCCP Section 1: Basic principles, laboratory tests and pleural procedures. Lung India. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11093145/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge