Necrotizing Fasciitis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Necrotizing fasciitis (NF) is a rapidly progressive, life-threatening soft tissue infection characterized by widespread fascial necrosis, severe systemic toxicity, and high mortality if not promptly recognized and treated. The condition commonly affects the extremities, perineum, and trunk and is often associated with diabetes mellitus, immunosuppression, trauma, or recent surgery. Early diagnosis remains challenging because initial clinical findings may resemble cellulitis or other superficial soft tissue infections.
We present the case of a 58-year-old male with poorly controlled diabetes mellitus who presented with severe pain, swelling, erythema, and fever involving the left lower limb. Clinical examination, laboratory investigations, and imaging findings raised suspicion for necrotizing fasciitis. Emergency surgical debridement, broad-spectrum intravenous antibiotics, intensive supportive care, and wound management resulted in gradual clinical recovery.
This case highlights the importance of early recognition, aggressive surgical intervention, multidisciplinary management, and prompt antimicrobial therapy in improving outcomes among patients with necrotizing fasciitis.
Introduction
Necrotizing fasciitis is a severe soft tissue infection involving the fascia and subcutaneous tissues with rapid progression to tissue necrosis, systemic toxicity, septic shock, and multi-organ dysfunction. Despite advances in medical care, mortality rates remain between 20% and 40%, particularly when diagnosis and treatment are delayed.
The infection may be polymicrobial (Type I) or monomicrobial (Type II), most commonly involving Group A Streptococcus, Staphylococcus aureus, anaerobes, Enterobacterales, and other opportunistic pathogens.
Several factors increase susceptibility to necrotizing fasciitis, including:
- Diabetes mellitus
- Chronic kidney disease
- Immunosuppression
- Obesity
- Peripheral vascular disease
- Alcohol abuse
- Malignancy
- Recent trauma or surgery
Important pathological mechanisms include:
- Rapid bacterial proliferation
- Production of tissue-destroying toxins
- Microvascular thrombosis
- Fascial necrosis
- Impaired tissue perfusion
- Systemic inflammatory response
Common clinical manifestations include:
- Severe pain disproportionate to physical findings
- Rapidly spreading erythema
- Swelling and edema
- Fever and chills
- Skin discoloration
- Bullae formation
- Crepitus
- Signs of sepsis
Early recognition and emergency surgical management are essential to reduce morbidity and mortality.
Case Report
Patient History
A 58-year-old male presented to the emergency department with:
- Severe pain in the left lower leg for 3 days
- Progressive swelling
- Redness of the affected limb
- High-grade fever with chills
- Difficulty walking
- Generalized weakness
The patient reported sustaining a minor abrasion to the lower leg one week prior while working outdoors. Initially, the wound appeared insignificant but progressively worsened.

Past medical history revealed:
- Type 2 diabetes mellitus for 12 years
- Hypertension
- Poor glycemic control
There was no history of:
- Recent surgery
- Deep vein thrombosis
- Autoimmune disease
- Malignancy
- Immunosuppressive therapy
Clinical Examination
General Examination
- Temperature: 39.2°C
- Pulse rate: 118/min
- Blood pressure: 96/62 mmHg
- Respiratory rate: 24/min
- Oxygen saturation: 95% on room air
The patient appeared toxic and dehydrated.
Local Examination
Examination of the left lower limb revealed:
- Diffuse swelling extending from ankle to knee
- Marked erythema
- Skin warmth
- Extreme tenderness
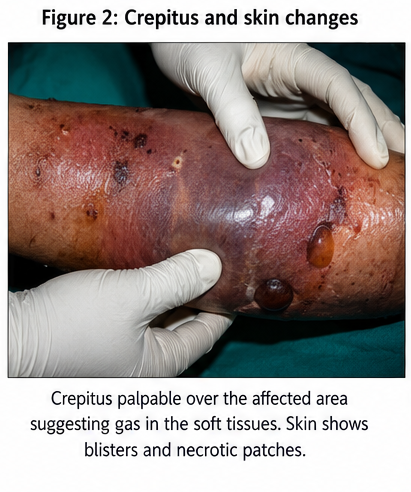
- Areas of dusky skin discoloration
- Multiple hemorrhagic bullae
- Foul-smelling serous discharge
Pain was disproportionately severe compared to visible skin findings.
Palpation demonstrated:
- Subcutaneous edema
- Areas of skin anesthesia
- Crepitus suggestive of gas-forming infection
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
- Severe cellulitis
- Deep vein thrombosis
- Gas gangrene
- Pyomyositis
- Necrotizing fasciitis
The rapid progression, severe pain, systemic toxicity, skin discoloration, and crepitus strongly suggested necrotizing fasciitis.
Investigations
Laboratory Findings
- White blood cell count: 24,500/mm³
- C-reactive protein: Markedly elevated
- Serum sodium: 130 mmol/L
- Serum creatinine: Elevated
- Random blood glucose: 312 mg/dL
- HbA1c: 9.8%
- Serum lactate: Elevated
Blood cultures were obtained before initiation of antibiotic therapy.
Imaging
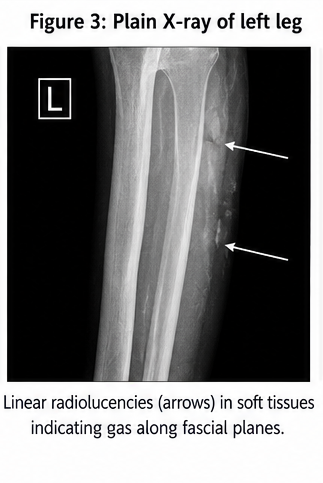
Plain Radiography
- Presence of soft tissue gas within fascial planes
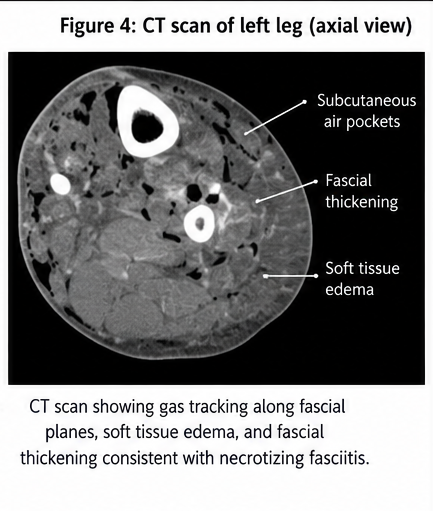
Contrast-Enhanced CT Scan
Findings included:
- Fascial thickening
- Extensive soft tissue edema
- Gas tracking along fascial planes
- Subcutaneous air pockets
These findings strongly supported the diagnosis of necrotizing fasciitis.
Microbiology
Tissue samples obtained during surgery demonstrated:
- Gram-positive cocci
- Mixed aerobic and anaerobic organisms
Culture later confirmed polymicrobial infection involving:
- Streptococcus pyogenes
- Escherichia coli
- Bacteroides species
Diagnosis
Based on clinical findings, laboratory abnormalities, imaging studies, and operative findings, a diagnosis of Acute Polymicrobial Necrotizing Fasciitis of the Left Lower Limb was established.
Management and Outcome
Initial Management
The patient was immediately admitted to the intensive care unit.
Resuscitative measures included:
- Intravenous fluid therapy
- Hemodynamic monitoring
- Glycemic control using insulin infusion
- Electrolyte correction
Broad-spectrum empirical antimicrobial therapy was initiated with:
- Piperacillin-tazobactam
- Clindamycin
- Vancomycin
Surgical Management
Emergency surgical exploration was performed within hours of diagnosis.
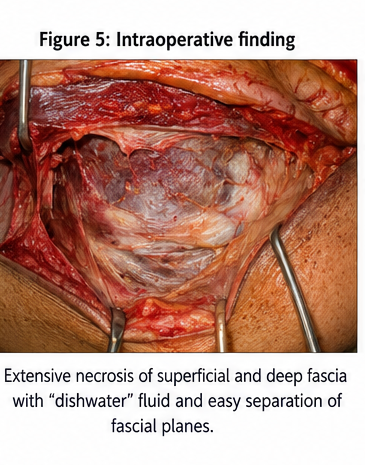
Intraoperative findings included:
- Extensive fascial necrosis
- Gray, nonviable tissue
- Thin foul-smelling exudate
- Easy separation of fascial planes
Aggressive surgical debridement was undertaken to remove all necrotic tissue.
The patient subsequently underwent two additional debridement procedures over the next week to ensure complete source control.
Follow-Up and Clinical Course
At 72 Hours
- Reduction in fever
- Improved hemodynamic stability
- Declining inflammatory markers
At 1 Week
- Healthy granulation tissue formation
- No further progression of infection
- Improved glycemic control
At 3 Weeks
- Wound bed suitable for reconstruction
- Split-thickness skin grafting performed
At 2 Months
- Complete wound healing
- Restoration of limb function
- No evidence of recurrent infection
The patient continued outpatient follow-up with surgical and diabetic care teams.
Discussion
Pathophysiology
Necrotizing fasciitis involves rapid destruction of fascia and subcutaneous tissues resulting from bacterial invasion and toxin production.
Key pathological processes include:
- Tissue ischemia
- Microvascular thrombosis
- Cytokine-mediated inflammation
- Fascial necrosis
- Systemic inflammatory response syndrome
Bacterial toxins contribute significantly to tissue destruction and systemic toxicity.
Epidemiology
Important epidemiological features include:
- Rare but highly fatal infection
- Incidence increasing worldwide
- More common in diabetic patients
- Higher prevalence among immunocompromised individuals
- Significant healthcare burden due to prolonged hospitalization
Clinical Manifestations
Common symptoms include:
- Severe pain
- Fever
- Swelling
- Rapid progression of skin changes
Characteristic signs include:
- Skin discoloration
- Bullae formation
- Crepitus
- Tissue necrosis
- Septic shock
Pain out of proportion to examination findings remains one of the earliest and most important clinical clues.
Diagnostic Considerations
Diagnosis is primarily clinical and should not be delayed while awaiting confirmatory investigations.
Useful diagnostic modalities include:
- Laboratory evaluation
- LRINEC scoring system
- Plain radiography
- Computed tomography
- Magnetic resonance imaging
- Surgical exploration
Surgical exploration remains the gold standard for definitive diagnosis.
Treatment Modalities
Surgical Therapy
The cornerstone of treatment includes:
- Immediate surgical exploration
- Aggressive debridement
- Repeat debridement when required
Delayed surgery significantly increases mortality.
Antimicrobial Therapy
Recommended broad-spectrum coverage should target:
- Streptococci
- Staphylococci
- Gram-negative organisms
- Anaerobic bacteria
Clindamycin is often added because of its toxin-suppressing effects.
Supportive Care
Supportive measures include:
- Intensive care monitoring
- Fluid resuscitation
- Vasopressor support when necessary
- Glycemic control
- Nutritional support
Complications
Potential complications include:
- Septic shock
- Multi-organ failure
- Limb loss
- Acute kidney injury
- Respiratory failure
- Prolonged hospitalization
- Death
Early intervention substantially reduces these risks.
Prognosis
The prognosis depends upon:
- Time to diagnosis
- Early surgical intervention
- Adequacy of debridement
- Presence of comorbidities
- Severity of sepsis
Patients receiving prompt surgical and medical management have significantly improved survival outcomes.
Conclusion
Necrotizing fasciitis is a rapidly progressive surgical emergency associated with significant morbidity and mortality. Early recognition of severe pain, rapidly spreading soft tissue infection, systemic toxicity, and characteristic skin findings is essential for timely diagnosis.
This case emphasizes the critical importance of prompt surgical debridement, broad-spectrum antimicrobial therapy, intensive supportive care, and multidisciplinary management in achieving favorable clinical outcomes. Early intervention remains the most important factor influencing survival and long-term functional recovery.
References
- Stevens DL, Bryant AE. Necrotizing Soft-Tissue Infections. https://pubmed.ncbi.nlm.nih.gov/29236909/
- Wong CH, Khin LW, Heng KS, Tan KC, Low CO. The LRINEC Score. https://pubmed.ncbi.nlm.nih.gov/15241098/
- Goh T, Goh LG, Ang CH, Wong CH. Early diagnosis of necrotizing fasciitis. https://pubmed.ncbi.nlm.nih.gov/22179937/
- Sartelli M, Guirao X, Hardcastle TC, et al. Management of skin and soft tissue infections. https://pubmed.ncbi.nlm.nih.gov/30737049/
- Centers for Disease Control and Prevention. Necrotizing Fasciitis. https://www.cdc.gov/group-a-strep/about/necrotizing-fasciitis.html
- World Health Organization. Sepsis and severe infections. https://www.who.int
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge