Lipoma: A Slowly Growing Benign Subcutaneous Soft Tissue Tumor of the Upper Back – A Case Report
OthersPage Navigation
Abstract
Lipoma is the most common benign mesenchymal soft tissue tumor composed of mature adipocytes enclosed within a thin fibrous capsule. It typically presents as a slow-growing, painless, soft, mobile subcutaneous mass and may occur anywhere in the body where adipose tissue is present. Although lipomas are generally asymptomatic, larger lesions may produce cosmetic concerns, discomfort, functional impairment, or compress adjacent structures. Accurate diagnosis through clinical examination and imaging is important to differentiate lipomas from other soft tissue tumors, including liposarcoma.
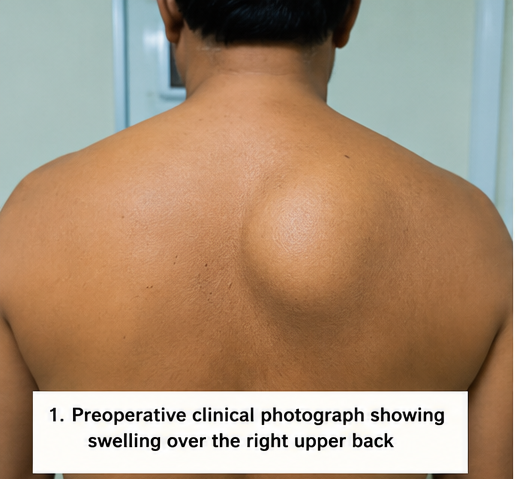
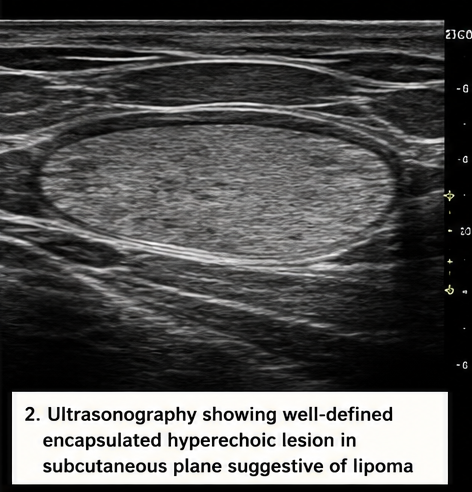
We report the case of a 45-year-old male who presented with a gradually enlarging swelling over the upper back for three years. Clinical examination revealed a soft, non-tender, mobile subcutaneous mass. Ultrasonography demonstrated a well-defined encapsulated fatty lesion suggestive of lipoma. Complete surgical excision was performed, and histopathological examination confirmed the diagnosis of conventional lipoma. The patient experienced an uneventful recovery with no recurrence during follow-up.
This case highlights the importance of thorough clinical assessment, imaging evaluation, and histopathological confirmation in the management of benign soft tissue tumors.
Introduction
Lipoma is a benign tumor arising from mature adipose tissue and represents the most frequently encountered soft tissue neoplasm in clinical practice. The incidence of lipoma is estimated to be approximately 1% of the general population, most commonly affecting adults between the fourth and sixth decades of life. These tumors are usually solitary but may occasionally occur as multiple lesions in conditions such as familial multiple lipomatosis, Dercum disease, and Madelung disease.
Lipomas can develop in various anatomical locations including the trunk, neck, shoulders, upper extremities, and thighs. Most lesions remain asymptomatic and are discovered incidentally during routine physical examination. The exact etiology remains unclear; however, genetic factors, minor trauma, obesity, and metabolic abnormalities have been proposed as contributing factors.
Common characteristics of lipoma include:
• Slow growth
• Soft consistency
• Painless nature
• Well-circumscribed margins
• Mobility over underlying structures
• Subcutaneous location
Although the diagnosis is often clinical, imaging modalities such as ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI) are useful in evaluating larger lesions and excluding malignant soft tissue tumors.
Case Report
Patient History
A 45-year-old male presented to the general surgery outpatient department with complaints of:
• Gradually enlarging swelling over the upper back
• Mild discomfort while lying supine
• Cosmetic concern due to visible swelling
• No associated pain
The patient first noticed a small swelling approximately three years earlier. The lesion had increased progressively in size but remained painless throughout its course. There was no history of rapid enlargement, skin ulceration, discharge, bleeding, fever, or weight loss.
The patient denied any history of trauma to the affected region.
Past medical history was unremarkable.
There was no history of:
• Diabetes mellitus
• Hypertension
• Tuberculosis
• Previous soft tissue tumors
• Malignancy
• Recent infections
Family history was non-contributory.
Clinical Examination
General physical examination was normal.
Vital signs were stable:
• Blood pressure: 126/80 mmHg
• Pulse rate: 78 beats/minute
• Respiratory rate: 16 breaths/minute
• Temperature: Afebrile
Local examination revealed:
• A solitary swelling over the right upper back
• Approximately 6 × 5 cm in size
• Oval-shaped appearance
• Smooth surface
• Soft consistency
• Well-defined margins
• Freely mobile over underlying structures
• Non-tender on palpation
• Normal overlying skin
No signs of inflammation, ulceration, or regional lymphadenopathy were present.
The lesion was clinically suggestive of a benign soft tissue tumor, most likely a lipoma.
Clinical Evaluation
Differential Diagnosis
The following differential diagnoses were considered:
• Lipoma
• Epidermoid cyst
• Sebaceous cyst
• Fibroma
• Neurofibroma
• Soft tissue sarcoma
• Liposarcoma
The characteristic soft consistency and mobility strongly favored lipoma.
Investigations
Laboratory Evaluation
Routine laboratory investigations were performed:
• Hemoglobin: 13.9 g/dL
• White blood cell count: 6,900/mm³
• Platelet count: 250,000/mm³
• ESR: 10 mm/hr
• Fasting blood glucose: 92 mg/dL
All laboratory parameters were within normal limits.
Ultrasonography
Ultrasonographic examination revealed:
• Well-circumscribed encapsulated lesion
• Homogeneous echogenic appearance
• Subcutaneous location
• Absence of internal vascularity
• No invasion of adjacent structures
The findings were highly suggestive of lipoma.
Magnetic Resonance Imaging
MRI was performed to further characterize the lesion.
Findings included:
• Well-defined subcutaneous mass
• Signal intensity identical to subcutaneous fat
• Thin fibrous capsule
• No evidence of infiltration
• No suspicious malignant features
Radiological findings were consistent with benign lipoma.
Diagnosis
Based on clinical examination and imaging findings, a provisional diagnosis of:
Conventional Subcutaneous Lipoma of the Upper Back was established.
Management and Outcome
Surgical Treatment
Considering the progressive increase in size and cosmetic concerns, complete surgical excision was planned.
Under local anesthesia:
• A linear skin incision was made
• The encapsulated lesion was identified
• Careful dissection was performed
• The tumor was completely excised
• Hemostasis was achieved
• The wound was closed in layers
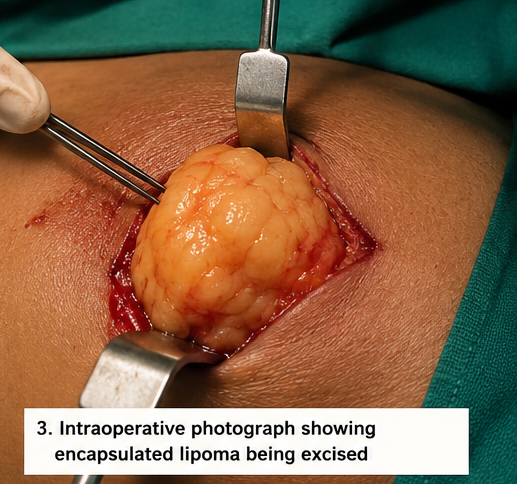
The excised specimen measured approximately 6.2 × 5.1 cm.

Gross Pathology
Macroscopic examination demonstrated:
• Yellow-colored soft tissue mass
• Lobulated appearance
• Thin fibrous capsule
• Uniform fatty consistency
Histopathological Examination
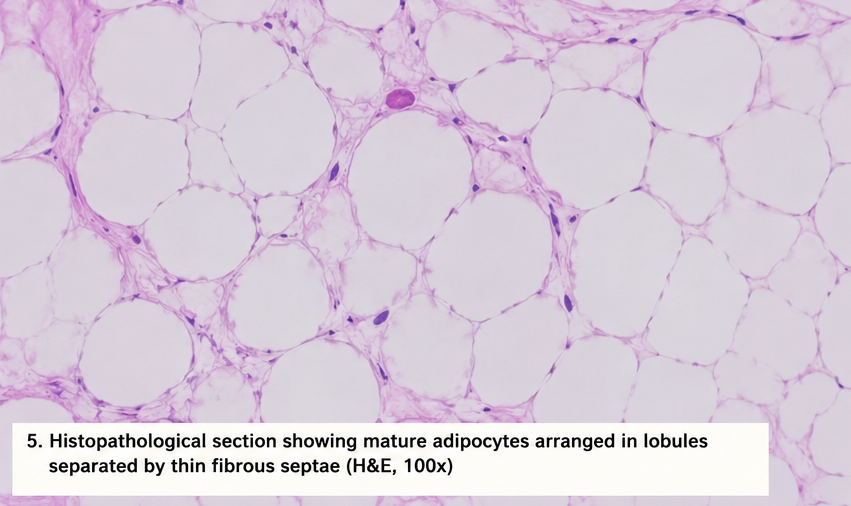
Microscopic evaluation revealed:
• Mature adipocytes arranged in lobules
• Thin fibrous septae
• Absence of cellular atypia
• No mitotic activity
• No necrosis
These findings confirmed the diagnosis of conventional lipoma.
Postoperative Course
The postoperative period was uneventful.
The patient was discharged on the same day with instructions regarding wound care and follow-up.
Follow-Up
At 2 Weeks
• Surgical wound healed well
• Sutures removed successfully
• No evidence of infection
At 3 Months
• Complete symptom resolution
• Excellent cosmetic outcome
• No recurrence
At 12 Months
• Patient remained asymptomatic
• No local recurrence
• Normal daily activities restored
Discussion
Lipomas are the most common benign tumors of adipose tissue and account for nearly half of all soft tissue tumors. They are composed of mature adipocytes enclosed within a delicate fibrous capsule and usually arise within subcutaneous tissue.
Although the precise pathogenesis remains uncertain, several theories have been proposed. Genetic abnormalities involving chromosome rearrangements, particularly involving chromosome 12q13–15, have been implicated in lipoma development. Obesity does not directly cause lipomas but may increase their visibility and clinical detection.
Clinical Features
Most lipomas present as:
• Soft painless masses
• Slow-growing lesions
• Mobile subcutaneous nodules
• Well-circumscribed swellings
• Solitary tumors
Common anatomical locations include:
• Neck
• Shoulder
• Upper back
• Trunk
• Forearm
• Thigh
Patients typically seek medical attention because of cosmetic concerns or gradual enlargement rather than pain.
Diagnostic Evaluation
Clinical examination remains the cornerstone of diagnosis. However, imaging studies are valuable in selected cases.
Ultrasonography provides:
• Rapid assessment
• Cost-effective evaluation
• Differentiation from cystic lesions
MRI is considered the imaging modality of choice for larger or deep-seated lesions because it accurately delineates tumor extent and helps distinguish benign lipomas from liposarcomas.
Differential Diagnosis
Several conditions may mimic lipoma clinically.
Epidermoid Cyst
Usually presents with a central punctum and firmer consistency.
Neurofibroma
Typically arises from peripheral nerves and may be associated with neurofibromatosis.
Fibroma
Characterized by firmer texture and fibrous composition.
Liposarcoma
Represents the most important differential diagnosis due to its malignant potential. Rapid growth, pain, deep location, and infiltrative features raise suspicion for malignancy.
Treatment
Management depends on lesion size, symptoms, and patient preference.
Treatment options include:
• Observation for asymptomatic lesions
• Surgical excision
• Liposuction-assisted removal
• Steroid injections in selected cases
Complete surgical excision remains the gold standard because it allows definitive diagnosis and minimizes recurrence.
Complications
Potential complications include:
• Cosmetic deformity
• Compression symptoms
• Local discomfort
• Infection
• Recurrence following incomplete excision
Malignant transformation of a conventional lipoma is exceedingly rare.
Prognosis
The prognosis of lipoma is excellent. Most patients experience complete cure following surgical excision. Recurrence rates are low when the lesion and capsule are entirely removed. Long-term outcomes are generally favorable with minimal morbidity.
Conclusion
Lipoma is the most common benign adipose tissue tumor and typically presents as a slow-growing, painless subcutaneous mass. Although diagnosis is often clinical, imaging studies play an important role in excluding malignant soft tissue tumors. This case illustrates the characteristic presentation, diagnostic evaluation, and successful surgical management of a conventional lipoma. Complete surgical excision remains the treatment of choice and provides excellent functional and cosmetic outcomes with minimal risk of recurrence.
References
- Kransdorf MJ. Benign soft-tissue tumors in a large referral population. AJR Am J Roentgenol. 1995;164(2):395–402. https://pubmed.ncbi.nlm.nih.gov/7839977/
- Bancroft LW, Kransdorf MJ, Peterson JJ, O'Connor MI. Benign fatty tumors: classification, clinical course, imaging appearance, and treatment. Skeletal Radiol. 2006;35(10):719–733. https://pubmed.ncbi.nlm.nih.gov/16802135
- Behr SC, Courtier JL, Qayyum A. Imaging of soft tissue tumors. Radiol Clin North Am. 2011;49(6):1197–1215. https://pubmed.ncbi.nlm.nih.gov/22024289/
- Medina CR, Schneider S, Mitra A, Spears J, Mitra A. Giant submental lipoma: case report and review of literature. Can J Plast Surg. 2007;15(4):219–222. https://pubmed.ncbi.nlm.nih.gov/19554182/
- Salam GA. Lipoma excision. Am Fam Physician. 2002;65(5):901–904. https://pubmed.ncbi.nlm.nih.gov/11898962/
- Rydholm A, Berg NO. Size, site and clinical incidence of lipoma. Acta Orthop Scand. 1983;54(6):929–934. https://pubmed.ncbi.nlm.nih.gov/6667119/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Researchers can now forecast how prostate cancer bone metastases will react to radium-223 treatment.
2.
Cardiopulmonary fitness is key for helping breast cancer patients manage post-diagnosis symptoms, say researchers
3.
In R/R Follicular Lymphoma, Tisa-Cel Produces Long-Lasting Responses.
4.
In MDS at Lower Risk, Novel Therapy Diminished Transfusion Dependency.
5.
WHO launches plan for free child cancer medicines
1.
Innovative Directions in Hematology Across Clinical Settings
2.
Transformative Approaches in Hematology for Healthcare Excellence
3.
How HLH is Revolutionizing Healthcare
4.
Essential Perspectives in Hematology and Patient Outcomes
5.
Neutrophil Profiling and AI Rewrites Cancer Diagnosis
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
An In-Depth Look At The Signs And Symptoms Of Lymphoma- The Q & A Session
2.
Navigating the Complexities of Ph Negative ALL - Part III
3.
Role of Nimotuzumab in Management of Nasopharyngeal Cancer
4.
Navigating the Complexities of Ph Negative ALL - Part X
5.
Management of 1st line ALK+ mNSCLC (CROWN TRIAL Update) - Part IV

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge