Thyroidectomy for Symptomatic Multinodular Goiter Causing Compressive Symptoms – A Case Report
OthersPage Navigation
Abstract
Multinodular goiter (MNG) is a common thyroid disorder characterized by diffuse enlargement of the thyroid gland with multiple nodules of varying size. Although many patients remain asymptomatic, progressive enlargement may lead to cosmetic deformity, dysphagia, dyspnea, voice changes, and compression of adjacent cervical structures. Thyroidectomy remains the definitive treatment for symptomatic multinodular goiter, especially when malignancy cannot be excluded or when compressive symptoms are present.
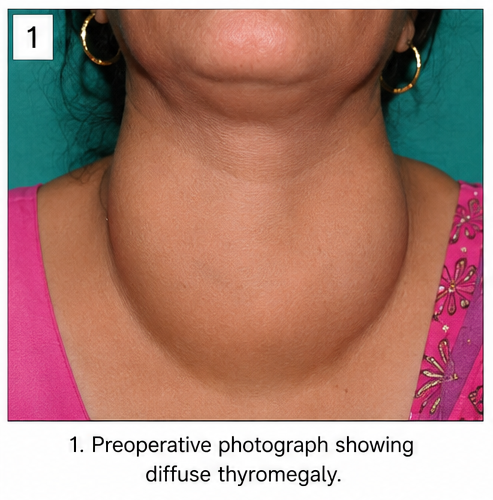
We report the case of a 52-year-old female who presented with a gradually enlarging anterior neck swelling associated with dysphagia and intermittent breathing difficulty. Clinical examination and radiological investigations revealed a large multinodular goiter causing tracheal deviation. Fine-needle aspiration cytology (FNAC) suggested benign nodular hyperplasia. Total thyroidectomy was performed successfully, and histopathological examination confirmed multinodular colloid goiter without evidence of malignancy. The patient recovered well postoperatively and remained symptom-free during follow-up.
This case highlights the importance of comprehensive evaluation and timely surgical management of symptomatic multinodular goiter to prevent progressive compressive complications and improve quality of life.
Introduction
Multinodular goiter is one of the most frequently encountered thyroid disorders worldwide. It is characterized by thyroid enlargement due to multiple hyperplastic nodules arising from repeated cycles of follicular epithelial proliferation and involution. The condition is more prevalent among women and older adults and may result from iodine deficiency, genetic predisposition, environmental factors, and hormonal influences.
Most multinodular goiters are benign and slow-growing. However, progressive enlargement can lead to significant compressive symptoms affecting the airway, esophagus, and recurrent laryngeal nerve. In addition, the possibility of occult thyroid malignancy necessitates careful evaluation.
Common clinical features of multinodular goiter include:
• Gradually enlarging neck swelling
• Visible thyroid enlargement
• Dysphagia
• Dyspnea
• Hoarseness of voice
• Cosmetic concerns
• Thyroid dysfunction in selected cases
Diagnostic assessment typically involves thyroid function testing, ultrasonography, fine-needle aspiration cytology, and cross-sectional imaging when substernal extension or airway compression is suspected.
Case Report
Patient History
A 52-year-old female presented to the endocrine surgery outpatient department with complaints of:
• Progressive swelling in the anterior neck
• Difficulty swallowing solid foods
• Occasional shortness of breath, especially when lying supine
• Cosmetic concern due to neck enlargement
The swelling had been present for approximately seven years and had gradually increased in size. During the previous six months, the patient noticed worsening dysphagia and intermittent breathing difficulty.
There was no history of:
• Significant weight loss
• Fever
• Neck pain
• Hemoptysis
• Previous neck irradiation
• Rapid increase in swelling size
Past medical history included controlled hypertension managed with oral medication.
There was no family history of thyroid cancer or endocrine disorders.
Clinical Examination
General physical examination was unremarkable.
Vital signs were stable:
• Blood pressure: 132/84 mmHg
• Pulse rate: 76 beats/minute
• Respiratory rate: 18 breaths/minute
• Temperature: Afebrile
Local examination revealed:
• Diffuse anterior neck swelling
• Enlargement involving both thyroid lobes
• Approximately 8 × 6 cm in size
• Multiple palpable nodules
• Firm but non-tender consistency
• Smooth overlying skin
• Movement with deglutition
No cervical lymphadenopathy was identified.
Mild tracheal deviation was noted clinically.
Clinical Evaluation
Differential Diagnosis
The following differential diagnoses were considered:
• Multinodular goiter
• Thyroid adenoma
• Thyroid cyst
• Hashimoto thyroiditis
• Follicular neoplasm
• Papillary thyroid carcinoma
• Medullary thyroid carcinoma
Investigations
Laboratory Evaluation
Routine laboratory investigations revealed:
• Hemoglobin: 13.5 g/dL
• White blood cell count: 7,400/mm³
• Platelet count: 268,000/mm³
• Serum calcium: 9.4 mg/dL
• Thyroid-stimulating hormone (TSH): 2.8 mIU/L
• Free T3: Within normal limits
• Free T4: Within normal limits
The patient was euthyroid.
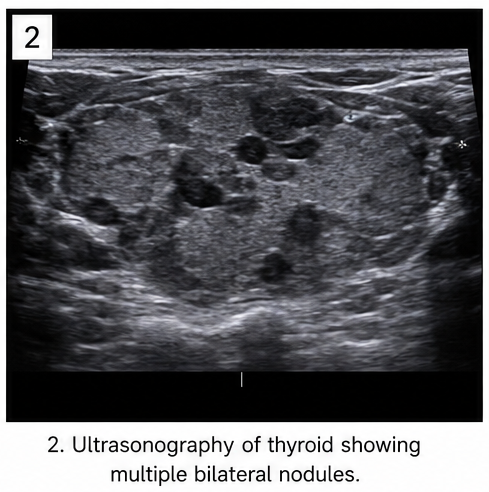
Ultrasonography
Neck ultrasonography demonstrated:
• Enlarged thyroid gland
• Multiple nodules involving both lobes
• Predominantly colloid appearance
• Largest nodule measuring 3.8 cm
• No suspicious microcalcifications
• No abnormal cervical lymph nodes
Fine-Needle Aspiration Cytology
FNAC performed from the dominant nodule revealed:
• Benign follicular cells
• Abundant colloid material
• No atypical or malignant cells
Findings were consistent with benign colloid nodular goiter.
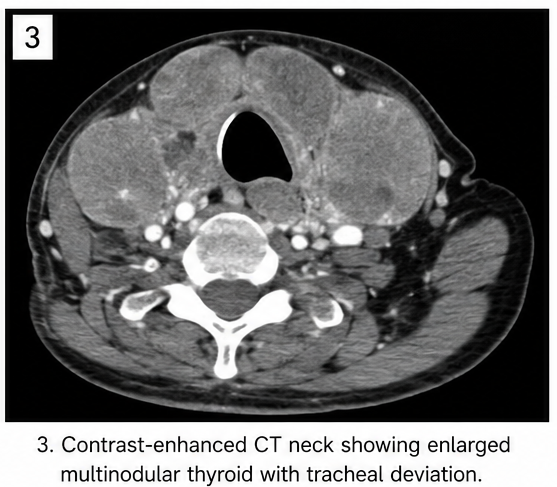
Computed Tomography
Contrast-enhanced CT of the neck demonstrated:
• Diffusely enlarged multinodular thyroid gland
• Mild tracheal deviation toward the right
• Minimal compression of the upper trachea
• No retrosternal extension
• No invasive features
Diagnosis
Based on clinical examination, imaging findings, and cytological evaluation, a diagnosis of: Symptomatic Multinodular Colloid Goiter with Compressive Symptoms was established.
Management and Outcome
Surgical Treatment
Considering the increasing compressive symptoms and progressive enlargement, total thyroidectomy was planned.
Under general anesthesia:
• A transverse cervical incision was made
• Subplatysmal flaps were elevated
• Strap muscles were separated
• Both thyroid lobes were mobilized carefully
• Recurrent laryngeal nerves were identified and preserved
• Parathyroid glands were preserved
• Total thyroidectomy was completed successfully
• Hemostasis was achieved
• A surgical drain was placed temporarily

Gross Pathology
The excised thyroid specimen demonstrated:
• Enlarged multinodular gland
• Multiple colloid-filled nodules
• Lobulated external surface
• No gross evidence of malignancy
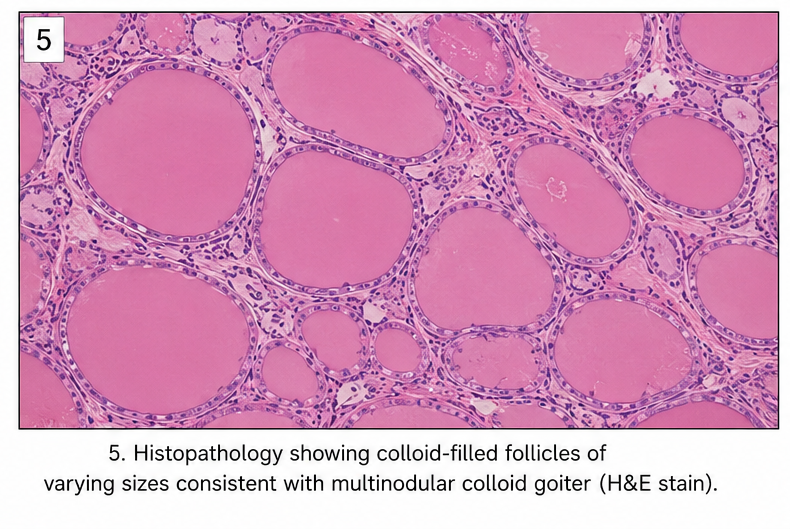
Histopathological Examination
Microscopic examination revealed:
• Hyperplastic thyroid follicles
• Variable-sized colloid-filled nodules
• Fibrous septations
• Areas of cystic degeneration
• Absence of capsular invasion
• No vascular invasion
• No malignant cells
Histopathological findings confirmed multinodular colloid goiter.
Postoperative Course
The immediate postoperative period was uneventful.
The patient remained hemodynamically stable.
Postoperative monitoring showed:
• Normal vocal cord function
• No evidence of recurrent laryngeal nerve injury
• Stable serum calcium levels
• No postoperative bleeding
The drain was removed on postoperative day two.
The patient was discharged on postoperative day three with levothyroxine replacement therapy.
Follow-Up
At 2 Weeks
• Surgical wound healed well
• No infection
• Normal voice quality
• No swallowing difficulty
At 3 Months
• Complete resolution of compressive symptoms
• Excellent cosmetic outcome
• Thyroid hormone levels within target range
At 12 Months
• Patient remained asymptomatic
• No recurrence
• Good quality of life
Discussion
Multinodular goiter represents a common cause of thyroid enlargement and remains a significant health problem worldwide. Although many patients remain asymptomatic for years, progressive gland enlargement can eventually result in compressive symptoms and cosmetic concerns that necessitate intervention.
Clinical Features
Common manifestations include:
• Neck swelling
• Dysphagia
• Dyspnea
• Hoarseness
• Tracheal deviation
• Cosmetic deformity
Most patients present after several years of gradual thyroid enlargement.
Diagnostic Evaluation
Evaluation of multinodular goiter requires a combination of clinical examination and diagnostic investigations.
Ultrasonography provides:
• Assessment of thyroid size
• Characterization of nodules
• Detection of suspicious features
• Evaluation of cervical lymph nodes
FNAC remains the primary method for excluding malignancy in dominant or suspicious nodules.
CT imaging is particularly useful when:
• Airway compression is suspected
• Retrosternal extension is present
• Surgical planning is required
Treatment
Management depends on symptom severity, thyroid function, and risk of malignancy.
Treatment options include:
• Observation
• Thyroid hormone suppression therapy
• Radioactive iodine therapy
• Hemithyroidectomy
• Total thyroidectomy
Total thyroidectomy is preferred for bilateral multinodular disease because it minimizes recurrence and provides definitive treatment.
Potential Complications
Complications following thyroidectomy include:
• Recurrent laryngeal nerve injury
• Hypocalcemia
• Neck hematoma
• Wound infection
• Voice changes
• Hypothyroidism
Meticulous surgical technique significantly reduces these risks.
Prognosis
The prognosis following thyroidectomy for benign multinodular goiter is excellent. Most patients experience complete resolution of compressive symptoms and significant cosmetic improvement. Long-term outcomes are favorable with appropriate thyroid hormone replacement and regular follow-up.
Conclusion
Multinodular goiter is a common thyroid disorder that may remain asymptomatic for years before producing compressive symptoms. Comprehensive clinical assessment, imaging evaluation, and cytological investigation are essential for accurate diagnosis and treatment planning. This case demonstrates the successful management of symptomatic multinodular goiter through total thyroidectomy, resulting in complete symptom relief and excellent postoperative outcomes. Early surgical intervention in appropriately selected patients can prevent progressive airway and esophageal compression while improving overall quality of life.
References
- Agarwal G, Aggarwal V. Is total thyroidectomy the surgical procedure of choice for benign multinodular goiter? An evidence-based review. World J Surg. 2008;32(7):1313-1324 https://pubmed.ncbi.nlm.nih.gov/18449595/
- Moalem J, Suh I, Duh QY. Treatment and prevention of recurrence of multinodular goiter: an evidence-based review of the literature. World J Surg. 2008;32(7):1301-1312. https://pubmed.ncbi.nlm.nih.gov/18305998/
- Medeiros-Neto G. Multinodular Goiter. In: Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2016. https://www.ncbi.nlm.nih.gov/books/NBK285569/
- Can AS, Peker K. Goiter. StatPearls Publishing. Updated 2023. https://www.ncbi.nlm.nih.gov/books/NBK562161/
- Zambudio AR, Rodríguez J, Riquelme J, Soria T, Canteras M, Parrilla P. Prospective study of postoperative complications after total thyroidectomy for multinodular goiters by surgeons with experience in endocrine surgery. Ann Surg. 2004;240(1):18-25. https://europepmc.org/article/med/15213613
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge