Eczema (Atopic Dermatitis) Presenting with Chronic Pruritic Erythematous Plaques and Recurrent Flares in a Young Adult: A Case Report
OthersPage Navigation
Abstract
Eczema, also known as atopic dermatitis, is a chronic inflammatory skin disorder characterized by intense pruritus, xerosis, recurrent eczematous lesions, and a relapsing-remitting clinical course. It affects individuals of all ages and significantly impairs quality of life due to persistent itching, sleep disturbances, and psychosocial stress. The disease results from a complex interaction between genetic susceptibility, epidermal barrier dysfunction, immune dysregulation, and environmental triggers. Early diagnosis and individualized management using skin hydration, trigger avoidance, topical anti-inflammatory therapy, and patient education remain the cornerstone of treatment. We report the case of a 24-year-old woman who presented with severe itching, dry skin, and recurrent erythematous plaques over the flexural aspects of both upper limbs and neck for six months. Clinical examination demonstrated excoriated eczematous plaques with lichenification. Laboratory investigations showed elevated serum IgE levels and mild peripheral eosinophilia. The patient was diagnosed with moderate atopic dermatitis and treated with regular emollients, topical corticosteroids, topical calcineurin inhibitors, oral antihistamines, and lifestyle modifications. Significant clinical improvement was observed within eight weeks, with sustained remission during follow-up. This case highlights the importance of early recognition, comprehensive patient education, and long-term skin barrier restoration in reducing disease recurrence and improving quality of life.
Introduction
Eczema, particularly atopic dermatitis, is one of the most common chronic inflammatory dermatological disorders worldwide. It affects approximately 15–20% of children and 2–10% of adults, with increasing prevalence in urban populations. The disease is characterized by chronic pruritus, xerosis, recurrent eczematous lesions, and periods of exacerbation and remission.
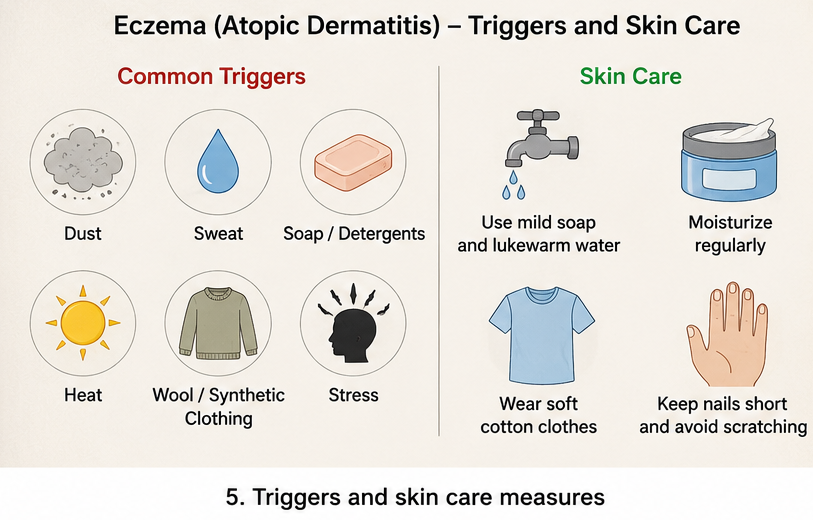
The pathogenesis involves epidermal barrier dysfunction, genetic abnormalities such as filaggrin gene mutations, immune dysregulation with predominant T-helper 2 (Th2) responses, altered skin microbiota, and environmental allergens. Common triggers include soaps, detergents, dust mites, pollen, sweating, stress, wool clothing, weather changes, and microbial colonization.
Patients typically present with severe itching, erythema, papules, vesicles, excoriations, scaling, and lichenification. Chronic scratching perpetuates the itch-scratch cycle, leading to worsening inflammation and skin thickening. Diagnosis is primarily clinical based on characteristic morphology, chronicity, distribution, and associated personal or family history of atopy.
Current treatment strategies emphasize restoration of the skin barrier using emollients, reduction of inflammation with topical corticosteroids or calcineurin inhibitors, avoidance of known triggers, treatment of secondary infection when present, and systemic therapy or biologics for severe disease.
Case Report
A 24-year-old woman presented to the dermatology outpatient department with complaints of persistent itching, dry skin, and recurrent reddish skin lesions affecting both antecubital fossae, neck, and wrists for approximately six months. The itching was severe, particularly during the night, resulting in disturbed sleep and reduced daily productivity. She reported that the symptoms worsened after exposure to dust, excessive sweating, hot weather, and the use of fragranced soaps.
The patient had experienced intermittent episodes of similar skin lesions since adolescence, with increasing frequency during the previous year. She also had a history of allergic rhinitis but denied asthma, food allergies, or recent medication use. There was a positive family history of atopic disease, with her mother suffering from allergic rhinitis.
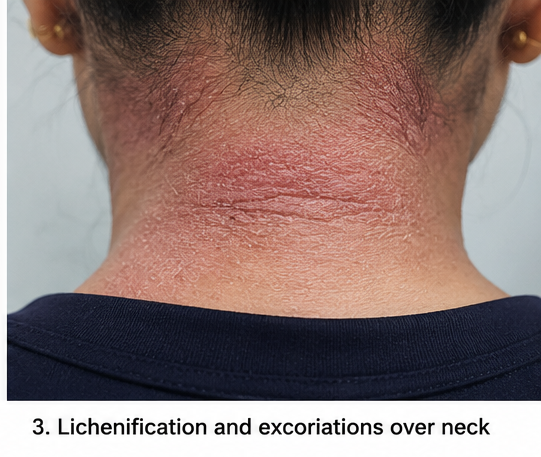
On physical examination, the patient appeared comfortable but frequently scratched the affected areas. Vital signs were stable. Dermatological examination revealed multiple poorly defined erythematous eczematous plaques involving both posterior neck, antecubital fossae, wrists, and popliteal fossae.
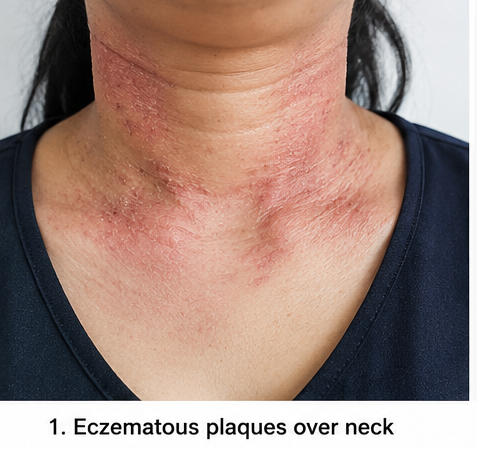

The lesions demonstrated excoriations, fine scaling, xerosis, and areas of lichenification secondary to chronic scratching.
No vesicles, pustules, or signs of bacterial superinfection were observed.
Laboratory investigations demonstrated mild peripheral eosinophilia with an eosinophil count of 8%, elevated total serum IgE level of 890 IU/mL, and normal complete blood count, liver function tests, renal function tests, and fasting blood glucose levels. Patch testing for common contact allergens was negative. Based on the clinical presentation, chronic relapsing course, flexural distribution, associated atopic history, and laboratory findings, a diagnosis of moderate atopic dermatitis (eczema) was established.
Management and Outcome
The patient received comprehensive management focusing on restoration of skin barrier function, reduction of inflammation, and prevention of disease recurrence.
She was advised to apply fragrance-free emollients liberally at least three to four times daily and immediately after bathing. A medium-potency topical corticosteroid was prescribed for active inflammatory lesions, while topical tacrolimus ointment was initiated for sensitive areas such as the neck to minimize long-term steroid exposure. Oral cetirizine was administered at bedtime to reduce nocturnal itching and improve sleep quality.

The patient received detailed counseling regarding avoidance of triggering factors, including harsh soaps, excessive bathing with hot water, synthetic clothing, dust exposure, and environmental irritants. She was encouraged to use mild soap substitutes, maintain short fingernails, wear loose cotton clothing, and regularly moisturize the skin.
Because no evidence of secondary bacterial infection was identified, systemic antibiotics were not required.
Within four weeks, itching had reduced considerably, erythema subsided, and the excoriations had healed. By eight weeks, significant improvement in xerosis and lichenification was observed, with restoration of normal daily activities and improved sleep. No treatment-related adverse effects occurred.
Follow-up
One Month
- Significant reduction in itching and erythema.
- Improved skin hydration with regular emollient use.
- Healing of excoriations without secondary infection.
- Better sleep quality and reduced scratching.
Three Months
- Near-complete resolution of inflammatory lesions.
- Marked improvement in lichenification.
- Minimal intermittent itching during weather changes.
- Continued maintenance therapy with moisturizers and topical tacrolimus.
Six Months
The patient remained clinically stable without major disease flare-ups. Skin hydration was well maintained, and only occasional mild itching occurred after exposure to known environmental triggers. She continued maintenance skin care with regular dermatological follow-up and remained free from significant complications.
Discussion
Atopic dermatitis is a multifactorial chronic inflammatory disorder in which impaired epidermal barrier integrity allows increased transepidermal water loss and penetration of allergens, microbes, and environmental irritants. This initiates immune activation dominated by Th2-mediated cytokines, including interleukin (IL)-4, IL-13, IL-31, and IL-5, resulting in persistent inflammation and severe pruritus.
The disease has a significant impact on physical and psychological well-being. Chronic itching often causes sleep disturbances, impaired work productivity, anxiety, depression, and reduced quality of life. Repeated scratching contributes to epidermal damage, lichenification, and an increased risk of secondary bacterial infections, particularly with Staphylococcus aureus.
Diagnosis remains largely clinical using standardized diagnostic criteria such as the Hanifin and Rajka criteria or the UK Working Party criteria. Laboratory investigations are supportive but not diagnostic, with elevated serum IgE and eosinophilia commonly observed in many patients.
The foundation of therapy is consistent restoration of the skin barrier through liberal use of moisturizers. Topical corticosteroids remain the first-line anti-inflammatory treatment during acute exacerbations, while topical calcineurin inhibitors are useful for sensitive areas and long-term maintenance. Oral antihistamines may improve sleep by reducing nocturnal pruritus, although they have limited effects on the underlying inflammatory process.
Patients with moderate-to-severe disease refractory to topical therapy may benefit from phototherapy, systemic immunosuppressive agents such as cyclosporine or methotrexate, or targeted biologic therapies including dupilumab and Janus kinase inhibitors. These therapies have transformed management in selected patients by providing sustained disease control while minimizing corticosteroid exposure.
Patient education remains one of the most important aspects of management. Identification and avoidance of individual triggers, adherence to moisturizing regimens, appropriate use of topical medications, and prompt recognition of disease flares significantly reduce recurrence and improve long-term outcomes.
Prognosis
The prognosis of eczema is generally favorable with appropriate long-term management. Many patients achieve good disease control through regular skin hydration, avoidance of triggering factors, and timely anti-inflammatory treatment. However, relapses remain common, particularly in genetically predisposed individuals or those exposed to persistent environmental triggers. Early diagnosis, patient education, adherence to maintenance therapy, and regular dermatological follow-up substantially improve quality of life and reduce disease severity over time.
Conclusion
Eczema is a chronic relapsing inflammatory skin disease that requires comprehensive long-term management rather than episodic treatment alone. Persistent pruritus, xerosis, and recurrent eczematous lesions should prompt early dermatological evaluation. Restoration of the skin barrier, individualized topical therapy, trigger avoidance, and patient education form the cornerstone of successful treatment. Early intervention and consistent maintenance therapy can effectively minimize disease flares, prevent complications, and significantly improve patient quality of life.
References
- Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. The Lancet. 2020;396(10247):345–360. https://pubmed.ncbi.nlm.nih.gov/32738980/
- Wollenberg A, Christen-Zäch S, Taieb A, et al. European guideline for atopic eczema. Journal of the European Academy of Dermatology and Venereology. 2018. https://pubmed.ncbi.nlm.nih.gov/29676534/
- Weidinger S, Novak N. Atopic dermatitis. The Lancet. 2016;387(10023):1109–1122. https://pubmed.ncbi.nlm.nih.gov/26377142/
- Eichenfield LF, Tom WL, Berger TG, et al. Guidelines of care for the management of atopic dermatitis. Journal of the American Academy of Dermatology. 2014. https://pubmed.ncbi.nlm.nih.gov/24290431/
- Bieber T. Atopic dermatitis. New England Journal of Medicine. 2008;358:1483–1494. https://pubmed.ncbi.nlm.nih.gov/18385500/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge